Healthy Hormones
Is your training in tune with your hormones and nutrition to optimise your athletic performance?
Hormones are internal chemical messengers regulating all aspects of your health and athletic performance. Discussed at recent BASEM conference “Health Hormones and Human Performance”

How? To enable your hormones to do the best job they can for your health and sport performance, you need to find a balance between what, how much and when you train, eat and sleep. In the diagram below, this represents staying on the healthy green plateau. Too much, or too little of any of these choices can lead to imbalances and tipping off the green plateau into the red, less healthy peripheries.

What? Imbalances between training load, nutrition and recovery can cause problems in the Endocrine system: the whole network of hormone interactions throughout your body. The bottom line is that if insufficient energy is provided through nutrition to cover both your training demands and the “housekeeping” activities within the body to keep you alive, then your body goes into energy saving mode. This situation is called relative energy deficiency in sports (RED-S) and has the potential to adversely impact one or more of the important systems in your body vital for optimal health and performance.
RED-S has evolved from the female athlete triad described in 1980s by Barbara Drinkwater in NEJM, where although female runners were consuming same dietary intake, those with higher training load were more likely to have menstrual dysfunction and low bone mineral density. Since this original description it has become obvious that the reproductive axis is just one of several hormone networks to be impacted by low energy availability and that RED-S also impacts the other half of the population: men.

Why? Suboptimal levels of energy availability to support health and performance can arise unintentionally, for example with increased training loads and/or times of growth and development in young athletes. Intentionally restrictive eating patterns can also be the cause of RED-S, particularly in sports/dance where low body weight confers a performance or aesthetic advantage. It is an indisputable fact that in order cycle up a mountain you need to overcome gravity and produce high watts/kg. Equally it is pretty impossible to do pointe work, let alone 32 fouttées en tournant en pointe unless you are a lightweight dancer. However if this at the expense of disrupting your hormones, then the advantage of being low body weight will be lost.
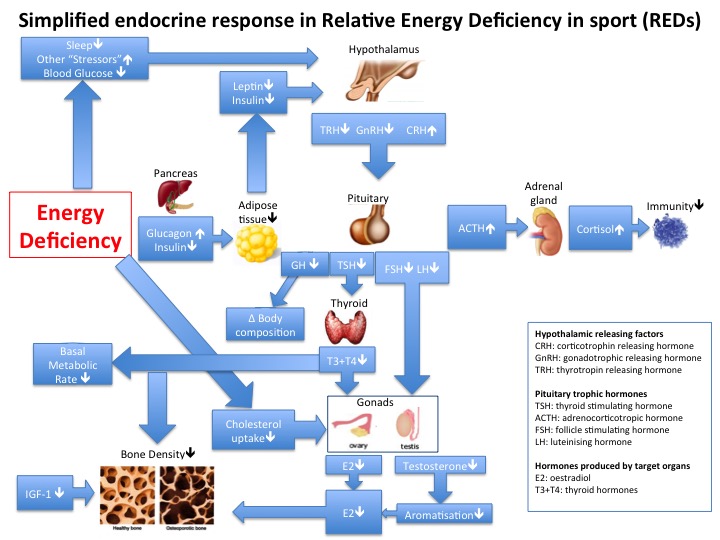
How to know? How to know if you, a teammate or a fellow athlete is at risk of RED-S? If you are a female athlete then your hormones are in balance if you are having regular periods (this does not include withdrawal bleeds as result of being on the oral contraceptive pill). Any woman of reproductive age from 16 years to the menopause should have regular periods (unless pregnant). Regular menstruation acts as the barometer of healthy hormones in women. If this is not the case, whether you are an athlete or not, you need to get this checked out medically to exclude underlying medical conditions. Having excluded these, then you need to review the integrated periodisation of training, nutrition and recovery. In male athletes there is not such an obvious sign that your hormones are at healthy levels. However recurrent injury/illness/fatigue can be warning signs. The diagram below shows all the potential adverse effects of RED-S on performance. Be aware that you do not have to have all, or indeed be aware of any of these effects if you develop RED-S.

So What? If you are an athlete/dancer, you may be thinking that none of this applies to you. You are feeling and performing fine. Maybe you have not yet experienced any of the detrimental effects of RED-S. However, you will never know how good an athlete you could be and whether you truly are performing to your full potential unless you put yourself in the best position in terms of your hormones to achieve this goal.

Key Points
• Insufficient nutrition intake (quantity and quality), whether intentional or not, results in RED-S and multiple hormonal disruptions
• RED-S has detrimental health and athletic performance consequences in both the short and the long term
• Some consequences of RED-S are irreversible for example poor bone health, unless intervention is swift
Check points
• Are you suffering with frequent injuries/fatigue/illness over last 3 months or more?
• Female athletes: if 16 years or older have your periods not started? Have you missed more than 3 consecutive periods?
If yes to any of above, seek medical advice from someone with experience Sports Endocrinology. Now! The longer you leave the situation the harder it will be to rectify. Initially underlying Endocrine conditions per se have to be ruled out. RED-S is a functional dysfunction of the Endocrine system, so a diagnosis of exclusion. Having established RED-S as the diagnosis, monitoring Endocrine markers can be very helpful as these are examples of objective metrics in monitoring energy availability and therefore response to optimising integrated periodisation of nutrition, training and recovery.

What to do? Don’t ignore! Although you may think you are fine, if your hormones are not working for you, then you will never reach your full potential as an athlete/dancer. For female athletes having regular periods means your hormones are in healthy ranges and this is normal. Not starting and/or missing periods is not healthy, for any woman.
For both male and female athletes, if you are experiencing recurrent injury, fatigue or illness, you need to get this checked out. There may be a simple explanation such as viral infection, low vitamin D or iron. However it may be that the underlying reason is due to hormone issues.
If you are an athlete, coach, teacher or parent and concerned that you/an athlete in your care has not got the balance right to optimise health and athletic performance, then a 3 way discussion will help and support the decision to seek medical advice as appropriate.
References
Lifestyle Choices for optimising health: exercise, nutrition, sleep Keay, BJSM 2017
Optimal health: including female athletes! Part 1 BJSM 2017
Optimal health: including male athletes! Part 2 BJSM 2017
Optimal Health: Especially Young Athletes! Part 3 BASEM 2017
Optimal Health: For All Athletes! Part 4 BASEM 2017
Low Energy Availability is Difficult to Assess But Outcomes Have Large Impact on Bone Injury Rates in Elite Distance Athletes Sport Nutrition and exercise Metabolism 2017
Cumulative Endocrine Dysfunction in Relative Energy Deficiency in Sport (RED-S) BJSM 2018
Presentation at BASEM conference “Health, Hormones and Human Performance”