Raising Awareness of RED-S in Male and Female Athletes and Dancers
Health4Performance is a recently developed BASEM open access educational resource
This is a world premier: a resource developed for and by athletes/dancers, coaches/teachers, parents/friends and healthcare professionals to raise awareness of Relative Energy Deficiency in Sport (RED-S)
What?
Optimal health is required to attain full athletic potential. Low energy availability (LEA) can compromise health and therefore impair athletic performance as described in the RED-S clinical model.
Dietary energy intake needs to be sufficient to cover the energy demands of both exercise training and fundamental physiological function required to maintain health. Once the energy demands for training have been covered, the energy left for baseline “housekeeping” physiological function is referred to as energy availability (EA). EA is expressed relative to fat free mass (FFM) in KCal/Kg FFM. The exact value of EA to maintain health will vary between genders and individuals, roughly equivalent to resting metabolic rate of the individual athlete/dancer. LEA for an athlete or dancer will result in the body going into “energy saving mode” which has knock on effects for many interrelated body systems, including readjustment to lower the resting metabolic rate in the longer term. So although loss in body weight may be an initial sign, body weight can be steady in chronic LEA due to physiological energy conservation adaptations. Homeostasis through internal biological feedback loops in action.
The most obvious clinical sign of this state of LEA in women is cessation of menstruation (amenorrhea). LEA as a cause of amenorrhoea is an example of functional hypothalamic amenorrhoea (FHA). In other words, amenorrhoea arising as a result of an imbalance in training load and nutrition, rather than an underlying medical condition per se, which should be excluded before arriving at a diagnosis of FHA. All women of reproductive age, however much exercise is being undertaken, should have regular menstrual cycles, which is indicative of healthy hormones. This explains why LEA was first described as the underlying aetiology of the female athlete triad, as women in LEA display an obvious clinical sign of menstrual disruption. The female athlete triad is a clinical spectrum describing varying degrees of menstrual dysfunction, disordered nutrition and bone mineral density. However it became apparent that the clinical outcomes of LEA are not limited to females, nor female reproductive function and bone health in female exercisers. Hence the evolution of the clinical model of RED-S to describe the consequences of LEA on a broader range of body systems and including male athletes.
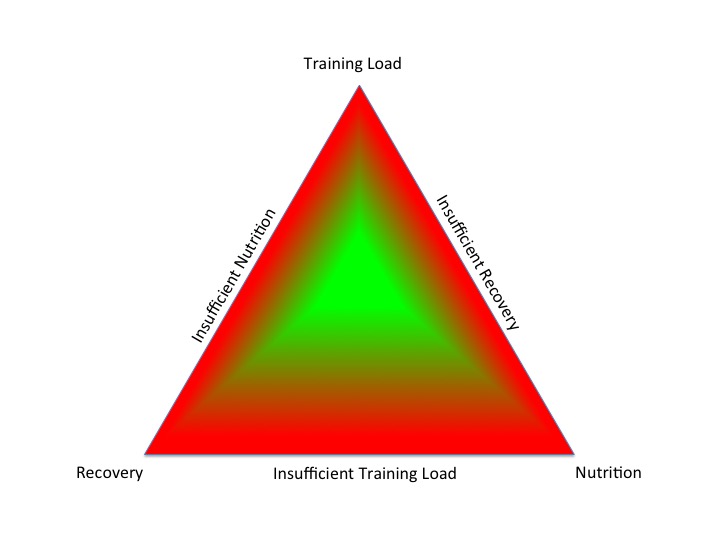
A situation of LEA in athletes and dancers can arise unintentionally or intentionally. In the diagram below the central column shows that an athlete where energy intake is sufficient to cover the demands from training and to cover basic physiological function. However in the column on the left, although training load has remained constant, nutritional intake has been reduced. This reduction of energy intake could be an intentional strategy to reduce body weight or change body composition in weight sensitive sports and dance. On the other hand in the column on the right, training load and hence energy demand to cover this has increased, but has not been matched by an increase in dietary intake. In both these situations, whether unintentional or intentional, the net results is LEA, insufficient to maintain health. This situation of LEA will also ultimately impact on athletic performance as optimal health is necessary to realise full athletic potential.

Although LEA is the underlying aetiology of RED-S, there are many methodological and financial issues measuring LEA accurately in “free living athletes“. In any case, the physiological response varies between individuals and depends on the magnitude, duration and timing of LEA. Therefore it is more informative to measure the functional responses of an individual to LEA, rather than the value calculated for EA. As such, Endocrine markers provide objective and quantifiable measures of physiological responses to EA. These markers also reflect the temporal dimension of LEA; whether acute or chronic. In short, as hormones exert network effects, Endocrine markers reflect the response of multiple systems in an individual to LEA. So by measuring these key markers, alongside taking a sport specific medical history, provides the information to build a detailed picture of EA for the individual, with dimensions of time and magnitude of LEA. This information empowers the athlete/dancer to modify the 3 key factors under their control of training load, nutrition and recovery to optimise their health and athletic performance.

Why?
Who is at risk of developing RED-S? Any athlete involved in sports or dance where being light weight confers a performance or aesthetic advantage. This is not restricted to elite athletes and dancers. Indeed the aspiring amateur or exerciser could be more at risk, without the benefit of a support team present at professional level. Young athletes are at particular risk during an already high energy demand state of growth and development. Therefore early identification of athletes and dancers at risk of LEA is key to prevention of development of the health and performance consequences outlined in the RED-S clinical model. Although there is a questionnaire available for screening for female athletes at risk of LEA, more research is emerging for effective and practical methods which are sport specific and include male athletes.
How?
Early medical input is important as RED-S is diagnosis of exclusion. In other words medical conditions per se need to be ruled out before arriving at a diagnosis of RED-S. Prompt medical review is often dependent on other healthcare professionals, fellow athletes/dancers, coaches/teachers and parents/friends all being aware and therefore alert to RED-S. With this in mind, the Health4Performance website has areas for all of those potentially involved, with tailored comments on What to look out for? What to do? Ultimately a team approach and collaboration between all these groups is important. Not only in identification of those at risk of LEA, but in an integrated support network for the athlete/dancer to return to optimal health and performance.
References
Heath4Performance BASEM Educational Resource
Video introduction to Health4Performance website
2018 UPDATE: Relative Energy Deficiency in Sport (RED-S) BJSM 2018
What is Dance Medicine? BJSM 2018
Identification and management of RED-S Podcast 2018
Low energy availability assessed by a sport-specific questionnaire and clinical interview indicative of bone health, endocrine profile and cycling performance in competitive male cyclists Keay, Francis, Hind. BJM Open Sport and Exercise Medicine 2018
How to Identify Male Cyclists at Risk of RED-S? 2018
Pitfalls of Conducting and Interpreting Estimates of Energy Availability in Free-Living Athletes IJSNM 2018
IOC consensus statement on relative energy deficiency in sport (RED-S): 2018 update BJSM 2018