Different Facets of the same Underlying Imbalances in Athlete Behaviours
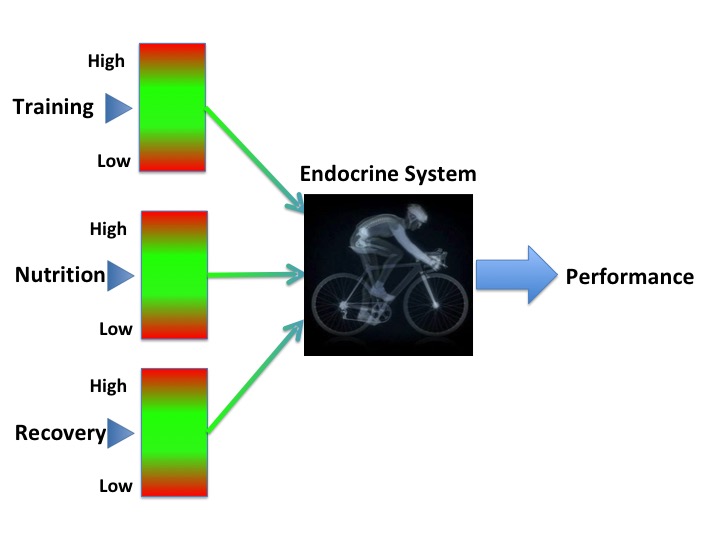
Although relative energy deficiency in sport (RED-S) and overtraining syndrome (OTS) are often described as distinct entities, these can be considered as different facets of the same unbalanced behaviours. For an exerciser these behaviours consist of exercise training load, nutritional intake and recovery.
What is RED-S?
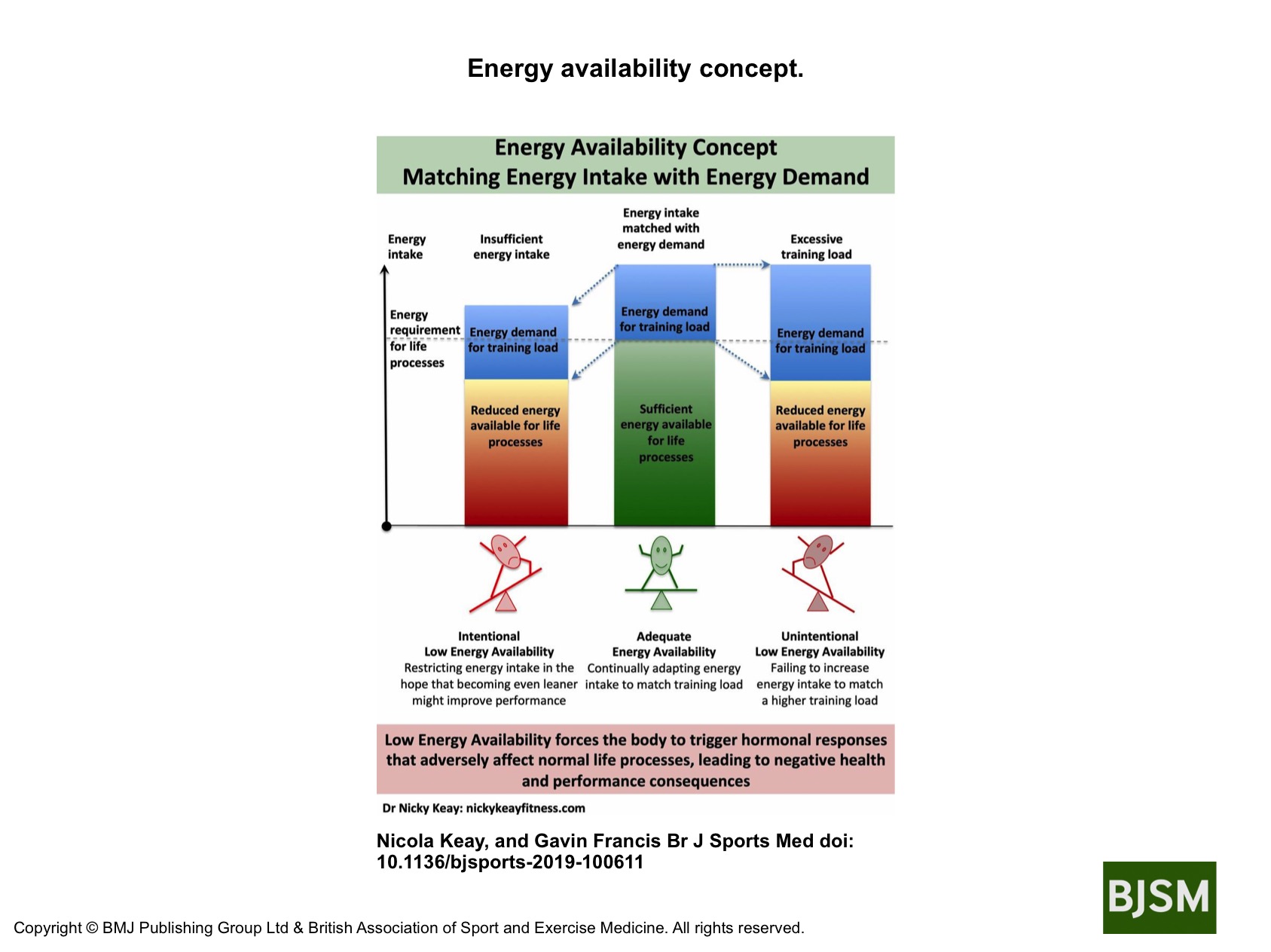
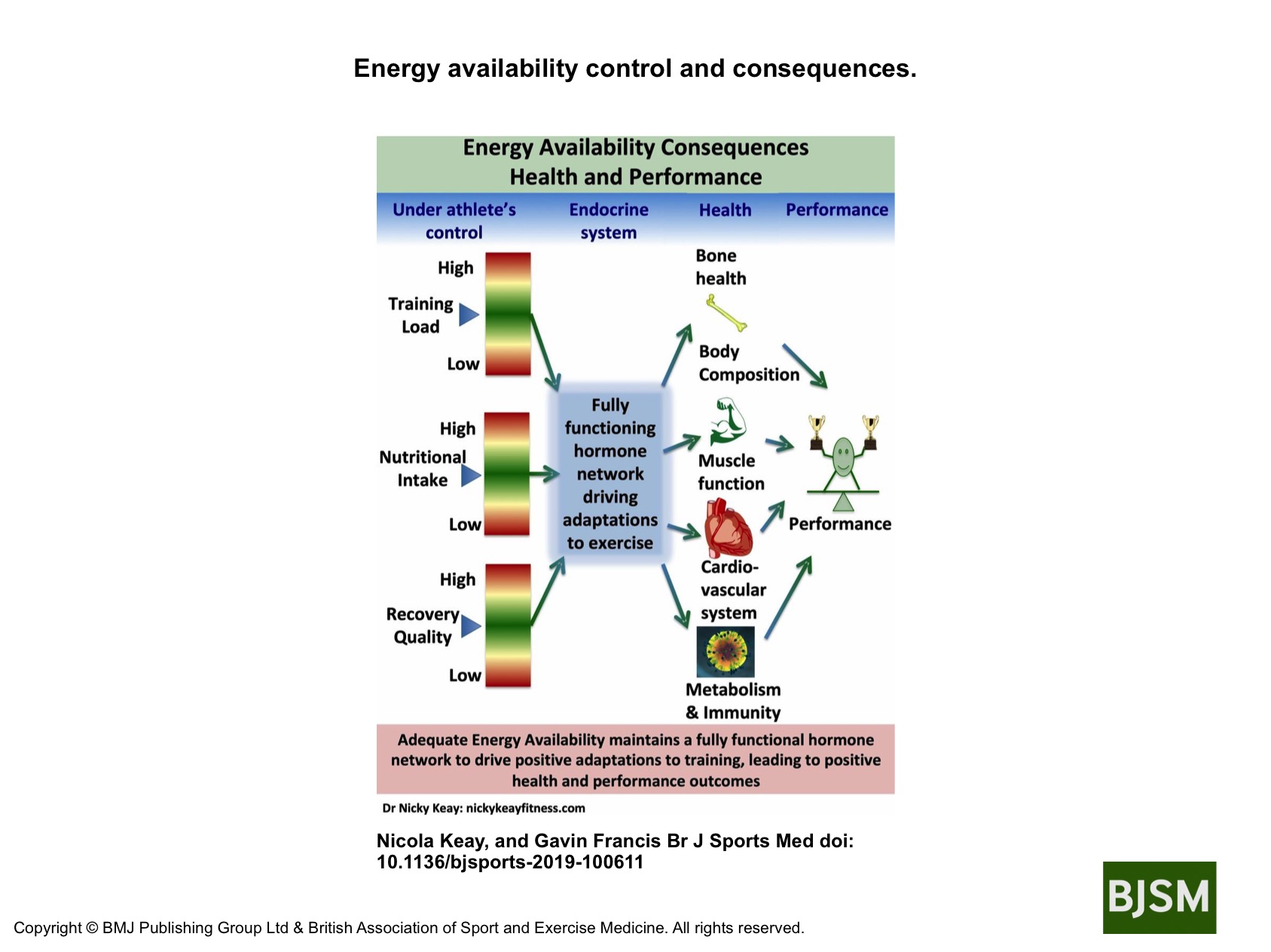
RED-S is a clinical syndrome describing adverse consequences in terms of health and performance due to sustained low energy availability (LEA). LEA is where there is a mismatch between energy intake and the combined energy demand from exercise and resting metabolic rate.
What is OTS?
OTS is a clinical syndrome describing adverse consequences in terms of health and performance when there is sustained non-functional overreaching (NFOR). NFOR is where there is an imbalance between training load relative to recovery.
It’s all about time scales
Thinking about RED-S and OTS in more detail, neither suddenly occur overnight. Rather it is the cumulative effect of energy deficit, or lack of recovery, that causes these syndromes over longer time scales of months.
Short time scales
Facets of LEA and NFOR
For example, the occasional day of suboptimal fuelling/high energy demand, with accompanying relative low energy availability, although not ideal, is nevertheless recoverable. This is shown by the warning masque of LEA of the rotating cube. On the opposite side is the warning masque of NFOR, where there have been some occasions of insufficient recovery over a short time scale of days. As with LEA, this is potentially a recoverable situation.
Longer time scales
Facets of RED-S and OTS
In practical terms, imagine you have been on a training camp or a dance intensive over a week or two. You may have unintentionally incurred a degree of LEA and NFOR, but if you take some time to rest and refuel afterwards, then you will be able to resume usual training fitter and stronger. On the other hand, if you continue to try and train at high intensity, in relative energy deficit you will progress after more weeks and months into the alert red masques of OTS and RED-S. In each case these outcomes are different facets of the same underlying imbalances in athlete/dancer behaviours around training load, nutrition and recovery.
Practical implications
When an athlete or dancer presents with symptoms that could include fatigue, poor sleep, menstrual disruption, recurrent injury (soft tissue or bone), digestive issues and other issues; it is very important to exclude medical conditions. Once this has been done and a diagnosis of exclusion made to confirm a functional issue, then deciding whether to use the terminology RED-S or OTS has a subtle nuance because in practice these syndromes are facets of the same underlying imbalance in athlete behaviours. In all cases the most important aspect is to outline a course of action for the athlete that includes training load, nutrition and recovery, in combination.
Athlete and dancer support
For example, athletes experiencing RED-S often ask if they can restore healthy hormone network function by simply eating more while maintaining a high training load. The simple answer is that this makes recovery less certain as a high training load, specifically high intensity, will most likely mean there is also a degree of NFOR. Therefore, adjustment in all athlete behaviours in synchrony is more effective for health and performance restoration. Similarly in an athlete experiencing OTS, in addition to reduction in training load, optimising nutritional intake will help.
Prevention is always better than cure
The prevention of adverse outcomes for the athlete or dancer is the other important practical implication of considering these clinical syndromes as facets of the same underlying issue. From the rotating cube of unbalanced athlete behaviours, LEA is the precursor to RED-S. Similarly, NFOR is the precursor to OTS. The progression in each case being determined by a longer time scale. Early identification of those at risk is essential to prevent this negative progression. Reversing the situation is a far easier task physiologically and psychological at an early stage of LEA and NFOR, rather than once in a “deeper hole” of RED-S or OTS.
Conclusions
RED-S and OTS being different facets of the same underlying issues of unbalanced athlete behaviours is a concept with practical implications.
References
Keay N. Hormones, Health and Human Potential. 2022 Sequoia books Act 1 Scene 9 “A Balancing Act” and Act 1 Scene 10 “In the Red”.




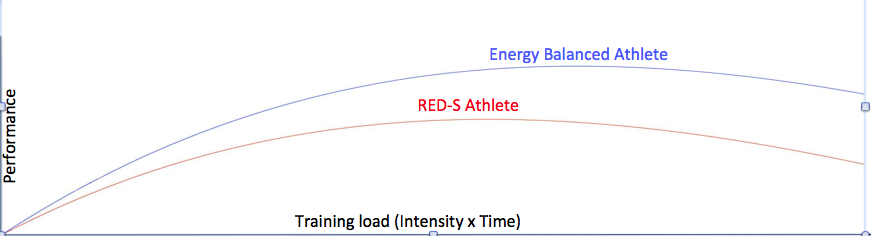 The Holy Grail of any training program is to improve performance and achieve goals.
The Holy Grail of any training program is to improve performance and achieve goals.