Introduction Relative Energy Deficiency in Sport (RED-S) has evolved from the previously described Female Athlete Triad (menstrual dysfunction, disordered eating and decreased bone mineral density). The reason for the development of this clinical model of RED-S is that it has become apparent that low energy availability, ie not eating enough calories to support the combined energy demands of health and training, has more widespread adverse impacts on health and consequently performance in athletes and dancers than previously recognised. Furthermore, the RED-S model includes both male and female athletes– so if you are a male athlete, please do not stop reading! Low energy availability can impact male and female exercises of all levels and of all ages. Young developing athletes can be at particular risk of RED-S as this represents a time of growth and development, which entails many nutritional demands, in addition to those to support training. This represents a time to set up the template for health into adulthood.
Why does RED-S occur? RED-S is particularly prevalent in sports where low body weight confers a performance advantage or for aesthetic reasons. For example: long distance running, triathlon, gymnastics, dance and cycle road racing. However, RED-S could also occur not as an intentional strategy to control body weight, but rather during cycles of increased training load where periodised nutrition has not been synchronised with the increased demand on the body.
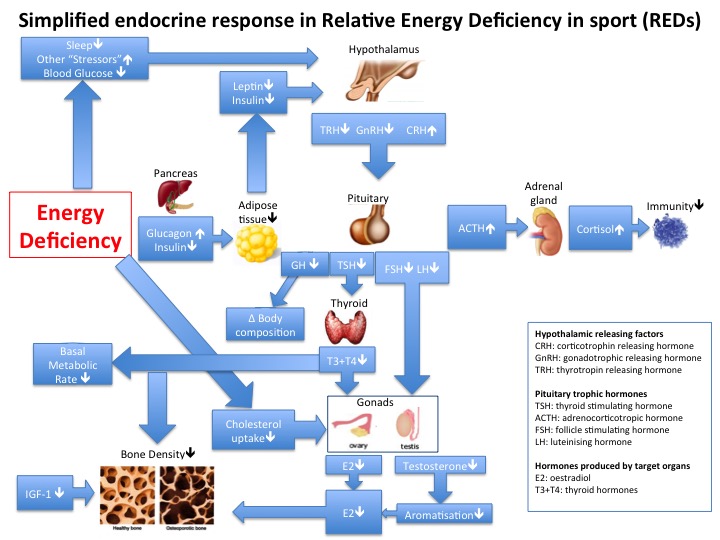
What is RED-S? Fundamentally there is a mismatch between food intake (in terms of energy and micronutrients) and the demand for nutrition required to cover expenditure, both of exercise training and for basic “housekeeping” tasks in the body to maintain health. If there is insufficient energy availability, then the body switches into an energy saving mode. This “go slow” mode has implications for hormone production and metabolic processes, which impacts all systems throughout the body. The reason why RED-S was originally described as the Female Athlete Triad is that in women the “energy saving mode” involves menstrual periods being switched off: a pretty obvious external sign as all women of child bearing age should have periods (apart from when pregnant). Low oestrogen levels have an adverse effect on bone health, resulting in decrease in bone mineral density. This effectively renders young women at increased risk of both soft tissue and bone injury, as seen in post-menopausal women. As described in the IOC statement published 2014 and updated 2018 in British Journal of Sports Medicine , the Female Athlete Triad is now recognised as just the tip of the iceberg. Disruption of hormone levels does not only adversely impact menstrual periods and bone health. There are knock on effects impacting the immune system, cardiovascular system, muscles, nervous system, gut health and the list goes on. Importantly, it is recognised that this situation is also seen in male athletes: low energy availability resulting in adverse health and performance consequences. Although exercise/dance is known to have many beneficial effects on health, all these beneficial effects are negated by low energy availability. For example, whether or not a sport is weight bearing, which traditionally improves bone health, in RED-S the predominant effect of disrupted hormones is to decrease bone density, leading to increased fracture risk.
Male cyclists Road cyclists are doubly at risk of the detrimental effects of RED-S on bone health. Performing a non-weight bearing form of exercise deprives the skeleton of the positive effect of mechanical skeletal loading on bone health. Furthermore being low body weight is a performance advantage for road cyclists when it comes to riding up hills/mountains in order to produce higher Watts/Kg over 60 minutes (60 minute functional threshold power FTP). This puts cyclists at risk of developing low energy availability, endocrine dysfunction and consequent impairment of bone health. In weight bearing sport the warning sign of suboptimal bone health if often stress fracture. This will be absent in cyclists. Hence low energy availability may go unrecognised until a bike fall results in serious fracture and indeed fractures appears as the most common type of injury amongst cyclists. Furthermore, the lumbar spine is recognised as the site most susceptible to endocrine dysfunction in RED-S. Vertebral fracture is recorded as the type of fracture in cyclists requiring the longest time off the bike. In a recent study, it was found that the factor most indicative of 60 minute FTP, was training load and NOT low body fat. Furthermore, training in low energy availability state will not result in the expected 60 minute FTP performance. So far more effective to train with sufficient nutrition on board, rather than restricting intake which will render training less effective.
What is the significance of RED-S? Do these effects of RED-S matter? Yes: there is a detrimental effect on not only health, but on all elements of sports performance. These include an inability to improve as expected in response to training and increased risk of injury. In the long-term there are potential implications for health with inability to reach peak bone mass for young athletes and at the other end of the scale, irreversible bone loss being seen in retired athletes.
Here is a summary of the potential impact of RED-S:
• Endocrine dysfunction: decreased training response
• Metabolic disruption: decreased endurance performance
• Bone health: increased risk bone stress injuries
• Decreased functional immunity: prone to infection
• Gut malfunction: impaired absorption of nutrients
• Decreased neuromuscular co-ordination: injury risk
• Psychological impact: inability to recognise risk developing RED-S
As you can see, these adverse effects are all relevant to performance in endurance sport.
What to do if you are concerned you may have RED-S?
Health Considerations:
• Women: even if your adult weight is steady, if you are a female athlete of reproductive age whose periods have stopped, then do not ignore this! In the first instance, you need to exclude any other causes (for example polycystic ovary syndrome and other hormone issues) in conjunction with your doctor. Then take a look at how you are eating in line with your training load – see the nutritional considerations section below.
• Men: if you are a male athlete struggling to improve sport performance, then review both your training load and your periodised nutrition and recovery. If the cause is RED-S then do not wait until your sport performance drops or you get injured before taking action. You may also want to consider having your testosterone levels measured to check that these are in the normal range.
Nutritional Considerations: From colleague Jo Scott-Dalgleish BSc (Hons), mBANT, CNHC
It is important to consider whether the energy deficiency that you are experiencing is intentional or unintentional.
Intentional: you may be deliberately restricting your calorie intake to lose weight and body fat, although you are already a healthy weight, as you believe this will improve your power-to-weight ratio or run speed.
- If you are trying to lose weight – or anxious about gaining weight – and experiencing issues with hormones (such as missing your periods or not experiencing morning erections) or bone health (such as getting a stress fracture) or finding that your performance is declining rather than improving, it may be time to seek support.
- This is particularly important if your eating patterns have become disordered, eg exclusion of multiple food groups, binge eating and/or purging, or deliberately avoiding social situations around food.
- Please visit the resources section of an excellent campaign website that has been put together to help athletes talk more openly about their experiences with food, disordered eating and RED-S and find help: https://trainbrave.org/resources/.
- Another great resource to learn more about RED-S and how it can adversely affect your health is http://health4performance.co.uk/athlete-dancer/
Unintentional: eating fewer calories than your body needs when you are training hard is common in endurance athletes and often not deliberate.
- You may not yet be experiencing the symptoms of RED-S outlined as above, but you are greatly at risk of doing so if you continue to under-eat relative to your training over a period of months or years.
- You do not need to be losing weight to be energy deficient, as your body’s metabolism adjusts to a lower intake but compromises on other functions while your weight stays the same. For example, you may experience constipation or bloating due to slowed digestive function. Here are some tips to help you meet your energy needs.
Here are some tips to help you to better manage your energy intake if you are at unintentional risk of RED-S.
- Track your food intake vs energy expenditure for a short period. Use My Fitness Pal or a similar app to track these daily over the course of week. On any day when you train, if you are consuming fewer than 2500 calories as a male endurance athlete and 2000 calories as a female endurance athlete after taking your energy expenditure through training into account, your intake is likely to be inadequate as these are the guidelines for the general population. Use this data to learn more about appropriate food choices and serving sizes and introduce some changes to increase your intake in line with your training load. But I do not suggest using apps like these on a long-term basis as they may encourage an unhealthy obsession with your food intake.
- Periodise your carbohydrate intake in line with your training. Increase your intake of starches and sugars (including vegetables and fruit) on your heavier training days. A low daily carbohydrate intake might be in the range of 2-4 g/kg of body weight. This is OK for lower volume training days but should be increased to 5-8 g/kg when training for 2-3 hours or more in a single day. This would include use of sports nutrition products like bars, gels and sports drinks during training. Again, use an app like My Fitness Pal for a week to help you assess your carbohydrate intake.
- Pay attention to your recovery nutrition. Consuming 15-25g of protein and 45-75g of carbohydrate in the hour after exercise, whether as a snack or as part of a meal will help you to each your energy intake goals, restock your glycogen stores for your next training session and protect lean muscle mass.
- Avoid excluding foods, whole food groups or following ‘fad diets’. Unless you have a genuine allergy or a diagnosed medical condition such as coeliac disease or lactose intolerance. Or you have been advised to avoid certain foods by a dietician or other well-qualified nutrition practitioner to help manage a health condition such as Irritable Bowel Syndrome. If you are vegetarian or vegan, see my blog here [link to https://www.endurancesportsnutritionist.co.uk/blog/vegan-diets-guide-endurance-athlete/] for tips on ensuring a well-balanced approach.
- Focus on nutrient density. Make good quality food choices to help you get enough vitamins and minerals as well as carbohydrates, protein, fat and fibre. Try to eat fresh, minimally processed foods rather than too much packaged food, including 3-5 servings of vegetables and 2-3 pieces of fresh fruit each day.
If you are experiencing relative energy deficiency, avoid following approaches like fasted training, where the training benefits are likely to be outweighed by the pitfalls of inadequate calorie intake. I also suggest avoiding low carb-high fat diets (LCHF) due to potential adverse effects on thyroid hormones, particularly T3, which may slow down metabolism and impact on performance. It can also be difficult to obtain adequate calories from these types of diets due to the near exclusion of a whole food group – which is why they may be very effective for weight loss in people who are overweight – and the lack of carbohydrate may harm performance through a loss of metabolic flexibility, ie ability to utilise carbohydrate as fuel when required for high intensity efforts.
Conferences in Sport/Dance, Exercise Science and Medicine 2018
References
Raising Awareness of RED-S in Male and Female Athletes and Dancers Dr N. Keay, British Journal of Sport Medicine 2018
2018 UPDATE: Relative Energy Deficiency in Sport (RED-S) Dr N. Keay, British Journal of Sport Medicine 2018
Low energy availability assessed by a sport-specific questionnaire and clinical interview indicative of bone health, endocrine profile and cycling performance in competitive male cyclists. Keay N, Francis G, Hind K. BMJ Open Sport & Exercise Medicine 2018
Optimal health: including female athletes! Part 1 Bones Dr N. Keay, British Journal of Sport Medicine 2017
Optimal health: including male athletes! Part 2 Relative Energy Deficiency in sports Dr N. Keay, British Journal of Sport Medicine 2017
Optimal Health: Especially Young Athletes! Part 3 – Consequences of Relative Energy Deficiency in Sports Dr N. Keay, British Association of Sport and Exercise Medicine 2017
Mechanisms for optimal health…for all athletes! Dr N. Keay, British Journal of Sport Medicine 2017
The IOC consensus statement: beyond the Female Athlete Triad—Relative Energy Deficiency in Sport (RED-S) British Journal of Sports Medicine 2014
Nutritional considerations for vegetarian endurance athletes Jo Scott-Dalgleish, Endurance Sports Nutrition 2017
 To recap, RED-S is a situation of low energy availability (LEA), which can lead to adverse health and performance consequences[3,4]. LEA can be a result of intentional energy restriction, which covers a spectrum of issues with eating from disordered eating to full blown clinical eating disorder. Ironically the original intention of these eating issues may have been to improve athletic performance, yet sustained LEA will ultimately lead to stagnation and deterioration in performance as found in male athletes[5].
To recap, RED-S is a situation of low energy availability (LEA), which can lead to adverse health and performance consequences[3,4]. LEA can be a result of intentional energy restriction, which covers a spectrum of issues with eating from disordered eating to full blown clinical eating disorder. Ironically the original intention of these eating issues may have been to improve athletic performance, yet sustained LEA will ultimately lead to stagnation and deterioration in performance as found in male athletes[5].