If you are striving to reach your peak performance, then the PEAQ can help you reach your personal full potential. Click here to get started on the PEAQ
Matching your energy intake to your energy demands helps you reach your personal peak health and exercise performance. On the other hand, failing to meet your energy demands results in low energy availability. This increases your risk of developing relative energy deficiency (REDs) and its adverse health and performance consequences.
People of any age, whatever their level and type of exercise, can be at risk of developing REDs; from elite dancers and athletes to recreational exercisers.
The PEAQ is a mobile Application that will guide you through a series of questions about exercise, physical characteristics, nutrition, hormone function and well-being. It just takes a few minutes.
Your PEAQ report instantly generates a REDs Risk Score and provides valuable insights into your energy status and potential risks, along with guidance. The PEAQ is intended for those 16 years of age and over.
The PEAQ has been developed based on in several published research studies where the questionnaire responses and scores have been correlated with measurements of hormones and bone health in athletes in various sports [1-7] and dancers [8-12]. These questionnaires were cited in the updated International Olympic Committee (IOC) consensus statement on REDs 2013.
Assessment of Relative Energy Deficiency in Sport, Malnutrition Prevalence in Female Endurance Runners by Energy Availability Questionnaire, Bioelectrical Impedance Analysis and Relationship with Ovulation status. Clinical Nutrition Open Science 2025S.
Body composition, malnutrition, and ovulation status as RED-S risk assessors in female endurance athletes, Clinical Nutrition ESPEN 2023, 58 :720-721
Keay N, Craghill E, Francis G Female Football Specific Energy Availability Questionnaire and Menstrual Cycle Hormone Monitoring. Sports Injr Med 2022; 6: 177
Nicolas J, Grafenuer S. Investigating pre-professional dancer health status and preventative health knowledge Front. Nutr. Sec. Sport and Exercise Nutrition. 2023 (10)
Nicola Keay, Martin Lanfear, Gavin Francis. Clinical application of monitoring indicators of female dancer health, including application of artificial intelligence in female hormone networks. Internal Journal of Sports Medicine and Rehabilitation, 2022; 5:24.
Nicola Keay, Martin Lanfear, Gavin Francis. Clinical application of interactive monitoring of indicators of health in professional dancers J Forensic Biomech, 2022, 12 (5) No:1000380
Mountjoy M, Ackerman KE, Bailey DM et al 2023 International Olympic Committee’s (IOC) consensus statement on Relative Energy Deficiency in Sport (REDs) British Journal of Sports Medicine 2023;57:1073-1098
This article explores the current state of play regarding relative energy deficiency in sport (REDs), highlighting the recent updates from the International Olympic Committee (IOC) consensus statement September 2023. Psychological factors and mental health are recognised as having a reciprocal relationship in both the aetiology and outcome of chronic low energy availability leading to REDs. This has important implications in terms of prevention and management of individuals experiencing REDs. Unintentional or intentional unbalanced behaviours around exercise and nutrition leads to a situation of low energy availability. Low energy availability is not synonymous with REDs. Rather cumulative, sustained low energy availability, particularly low carbohydrate availability, leads to the clinical syndrome of REDs comprising a constellation of adverse consequences on all aspects of health and performance. This situation can potentially arise in both biological sexes, all ages and level of exerciser. This is of particular concern for the young aspiring athlete or dancer, where behaviours are being established and in terms of long-term consequences on mental and physical health. The mechanism of sustained low energy availability leading to these negative health outcomes is through the adaptive down regulation of the endocrine networks. Therefore, raising awareness of the risk of REDs and implementing effective prevention and identification strategies is a high priority.
Introduction
Relative energy deficiency in sport (REDs) was first described in the International Olympic Committee (IOC) consensus statement published in the British Journal of Sports and Exercise Medicine (BJSM) 2014(Mountjoy, 2014). Since then, there have been updates published in 2018 (Mountjoy, 2018) and most recently in September 2023 (Mountjoy, 2023).
Seminal studies of female collegiate runners in 1980s found that those athletes with higher weekly training load, but same food intake as those with lower training load, experienced menstrual disruption, including secondary amenorrhoea and poor bone health (Drinkwater, 1984). This led to the description of the female athlete triad, which comprises a clinical spectrum of eating patterns, menstrual function and bone health. This ranges from optimal fuelling, menstrual function and bone health; to eating disorders, amenorrhoea and osteoporosis.
However, with further evidence emerging it became apparent that the impact of under fuelling is not confined to menstrual and bone health. Rather that the consequences of under fuelling are multisystem and can include male athletes. This led to the initial description of REDs in 2014 as a syndrome comprised of the potential adverse effects on many systems in the body with both physical and mental health implications. Crucially, unlike the female athlete trad, REDs also included the potential negative sequalae on athletic performance. Ultimately the goal for all athletes is to perform to their best, so REDs is not something of interest just in academic or clinical circles. REDs is highly relevant to both biological sexes and all levels and ages of exerciser.
What is Energy Availability?
The underlying aetiology of REDs is low energy availability. The life history theory describes how biological processes compete for energy resources (Shirley, 2022). Energy requirement for movement is prioritised from an evolutionary point of view in order to take evasion action from predators. The residual energy from food intake is described as energy availability. This is roughly equivalent to resting metabolic rate for the individual. Simply lying in bed all day, staying alive, is high energy demand for humans as homeotherms. The numerical value of energy availability is expressed in Kcals/Kg of fat free mass. The energy availability requirement for health will vary between individuals depending on sex, age and body composition. Although energy availability is a very useful concept, in practice is it not actually measured outside of the research setting. Rather objective surrogates indicating energy availability can be measured such as triiodothyronine (T3) which is used as a primary indicator of low energy availability as outlined in the update REDs clinical assessment tool described in further detail below (Stellingwerff, 2023 ).
An important highlight from the updated consensus statement on REDs is that it is specifically low carbohydrate availability that is most detrimental, especially for reproductive hormone networks. Comparing isocaloric intake, where there is a low proportion of energy from carbohydrate, this has the most marked negative consequence on both hormone health and performance. The mechanism of sustained low carbohydrate availability appears to involve the hormone leptin, an adipokine, secreted by adipose tissue. Low levels of leptin cause suppression of the reproductive axis via the hypothalamus-pituitary axis (Keay, 2022).
Aetiology of Low Energy Availability
Low energy availability is a situation where, once energy demand from movement has been met, the residual energy available is insufficient to support the functioning of other biological life process.
Low energy availability could arise unintentionally or intentionally (Keay, 2019). Unintentional low energy availability is where an exerciser does not appreciate the energy demands of exercise and other activities with an energy demand. For example, many athletes will not consider the energy required to “commute” to a training session on foot or bike. Unintentional low energy availability could be due to practical issues: for example, a long cycle ride over several hours will require the cyclist to take nutritional sources in the pockets of clothing and/or plan ahead suitable stops where it is possible to obtain nutrition. Similarly, going on a training camp, especially at altitude, will greatly increase energy demand from exercise and needs to factored in. Finances could also be a limiting factor.
On the other hand, intentional low energy availability is where an exerciser intentionally restricts nutrition intake in the belief that this might confer a performance advantage in terms of body weight, composition or shape. This is particularly associated with any exercise against gravity such as running, road cycling, climbing; weight category sports like martial arts and aesthetic forms of sport (diving, gymnastics) and dance.
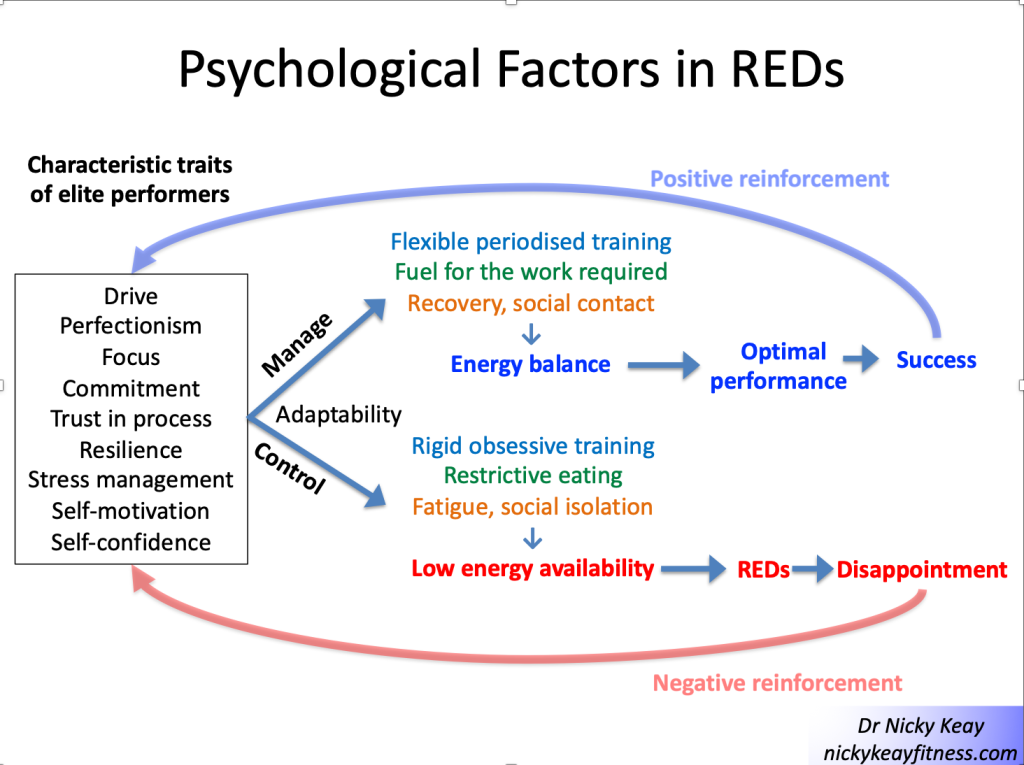
For individuals with intentional low energy availability, psychology and mental health can have a reciprocal interaction (Pensgaard, 2023). Those exercisers with personality characteristics such as self-motivation, perfectionism can be very laudable traits in terms of dedication to exercise training to achieve success. However, when these characterises impact and support rigid behaviours around training and nutrition, this can become problematic. This is shown in Figure 1 “Psychological factors in REDs”. Those who are able to adapt to external pressures and have a flexible approach to training and nutrition are more likely to experience positive outcomes. Whereas those who have a more rigid approach, which might include disordered eating and or an eating disorder and/or exercise dependence are more likely to experience negative outcomes. This reinforces self-doubt and culminates in a vicious circle of perpetuating rigid behaviours and negative outcomes in terms of both physical and mental health.
Evidence for this interaction between psychological factors and risk of REDs was found in our study of dancers, referenced in the updated IOC consensus statement. A significant relationship was found between psychological factors such as anxiety around body shape/weight and missing training. These psychological factors in turn had significant associations between physical manifestations of low energy availability (low body weight) and physiological outcomes (menstrual irregularity) (Keay, 2020). Similarly, in more of our published research papers referenced in the IOC consensus statement focusing on male athletes, an significant association was found between cognitive nutritional restraint and negative physiological and performance outcomes (Jorov, 2021).
This reciprocal interaction between internal and external factors is a systems biology approach, highlighted in the recent updated IOC consensus statement. From a physiological point of view the brain is a high energy demand organ, requiring a good supply of glucose. So low carbohydrate availability will restrict this cerebral supply, which can impair cognitive function and ultimately good decision making. It is interesting to reflect that the neuroendocrine gatekeeper, the hypothalamus keeps a watching brief on internal and external factors, not distinguishing between the source of stressors when putting in motion an adaptive response (Keay, 2022).
Consequences of Low Energy Availabiity
Low energy availability is not synonymous with REDs. Indeed, short term low energy availability might initially bring some good performances. Low energy availability becomes problematic depending on the time scale, which in turn determines the degree of adaptive response, described in the clinical physiological model of REDs (Burke, 2023). The first system to adapt to low energy availability is bone: bone turnover moves in favour of resorption over formation. This is why bone stress responses, specifically bone stress fractures, can be an early warning sign of REDs and designated a primary indicator in the updated IOC consensus statement. There will follow sequential down regulation of metabolic rate mediated via the thyroid axis, followed by the reproductive axis. In women primary amenorrhoea or sustained functional hypothalamic amenorrhoea (FHA) of 6 months or more duration is a severe primary indicator of REDs. In men, low rage testosterone is a severe primary indicator. Ultimately body composition will be adversely affected, with the only endocrine system to be up regulated being that of the hypothalamic-pituitary-adrenal axis (Keay, 2019).
Health
Cumulative low energy availability causes the syndrome of REDs, which produces progressive adverse effects on all aspects of health: physical, mental and social, described in the REDs conceptual model. Poor sleep will compound these negative health effects (Keay, 2022).
Performance
Although there may be some initial good performances, chronic low energy availability will result in adverse performance consequences of REDs, described in the REDs performance conceptual model. In our referenced papers in the consensus statement, we found that in male athletes, short term low energy availability impacted performance (Jurov, 2022). In another of our referenced studies we showed that male cyclists in sustained low energy availability over 6 months, not only experienced bone loss commensurate to astronauts in space, but these cyclists also underperformed compared to their energy replete fellow cyclists (Keay, 2019). On a positive note, explaining to athletes and dancers that improving energy availability will improve their performance, can help in overcoming problematic behaviours.
Identification of those at risk
In view of the potential adverse health and performance effects of REDs, it is a priority to raise awareness of this risk to affect prevention. To this end the British Association of Sports and Exercise Medicine (BASEM) has a website health4performance.co.uk dedicated to providing reliable information on REDs for athletes, parents, coaches and health care professionals together with BASEM endorsed online courses. Targeting and identifying those at increased risk is very important. Young athletes and dancers can be most severely affected as down regulation of hormone function due to low energy availability can cause delay in growth and development. In particular, delayed puberty and menarche dampens the accrual of peak bone mass, with implications for bone health (Keay, 2000). Furthermore, there is evidence that these adverse effects on bone health might not be fully reversible (Keay, 1997)
From a psychological point of view, the young aspiring athlete and dancer is also at heightened risk. Explored and viewed by many dancers in “The Dark Side of Ballet Schools” Panorama (season 33, episode 28). Selection for specialised training will inevitably favour those who are self-motivated and dedicated. In a group of individuals sharing similar psychological traits this could act as a “breeding ground” for reinforcing these characteristics in ways that could lead to behaviours which are not conducive to positive outcomes. Rather reinforcing the negative interpretation of external and internal factors, leading to a vicious circle of reinforcing attitudes and behaviours leading to REDs, as described in Figure 1
Risk stratification
Early identification of those at risk of developing REDs is an important preventative strategy. Especially for young aspiring athletes and dancers where behaviours around eating and exercise are being developed and established. A step-by-step approach is provided in the updated version 2 of the Relative Energy Deficiency in sport Clinical Assessment Tool (REDsCat v2) to identify and risk stratify individuals (Stellingwerff, 2023 ). Initial, low cost, screening questionnaires can be helpful, particularly if tailored to a specific sport/activity or dance. For example: sports specific energy availability questionnaire (SEAQ) (Keay, 2018) and dance energy availability energy questionnaire (DEAQ) (Keay, 2020). This can be helpful in identifying those individuals where further investigation is clinically indicated. As REDs is a diagnosis of exclusion, targeted blood testing excludes medical conditions per se and provide objective quantification in the stratification of risk. Severe primary indicators of REDs are issues in the reproductive axis: long duration of amenorrhoea in females and low range testosterone in males.
From a combination of all these results the individual can be placed in an appropriate risk category. The updated REDs CAT v2 includes a finer grained approach with four categories from green, yellow, amber to red.
This assessment also provides the background on which to base the appropriate level of support. For all, management will be directed at restoring energy availability and include modification of training and nutritional intake. However, the details will vary according to the severity of REDs. Individuals with intentional REDs, especially when formally diagnosed with an eating disorder, will need most intensive input than a person with transient unintentional low energy availability.
Management
A nuanced approach is required for individual athletes, depending on their risk stratification and biopsychosocial factors. In all cases some degree of psychological support will be helpful. Involvement of the extended multidisciplinary team is ideal: medical doctor, dietician, coach and parent (where appropriate) with the athlete/dancer at the centre.
In order to restore energy availability this will require careful discussion around nutrition in terms of consistency of eating patterns and composition of food groups consumed. This starts with regular meals containing good portions of complex carbohydrate and protein. Studies show that inconsistent intake of carbohydrate (eg “backloading” eating to the evening) produces an unfavourable hormone profile. Fuelling around training is also a high priority for hormone health and driving positive adaptations to exercise. Pre training consumption of carbohydrate together with post training refuelling with both complex carbohydrate and protein within 20 minutes of stopping are important behaviours for favourable hormone response to exercise (Keay, 2022).
In terms of pharmacological intervention, NICE guidelines have been updated 2022 in recommending body identical hormone replacement therapy (HRT) over the combined oral contraceptive pill (COCP) for bone protection in those with evidence of bone poor health due to functional hypothalamic amenorrhoea (FHA) as a consequence of REDs (BASEM, 2023). Poor bone health is defined as age matched Z score < -1 of the lumbar spine (trabecular bone particularly sensitive to low oestradiol) and/or 2 or more stress fractures at a site of concern (trabecular rich bone). For male athletes/dancers external testosterone is not appropriate as this supresses internal hormone production. Furthermore, testosterone is on the world anti-doping authority (WADA) banned list and it is not possible to obtain a therapeutic use exemption (TUE) as REDs is a functional condition, not a medical condition.
Prevention
Prevention is always the ultimate goal. In order to achieve this aim, a cultural shift in sport and dance is required. Emphasis on the fact that health is a prerequisite for performance. Pursuing a lighter body weight or leaner body composition will not automatically lead to improved performance. Each individual will have a personal tipping point. As we are all different, there is no such thing as a generic “ideal” weight/shape/body composition.
In practical terms, prevention can be considered as primary, secondary and tertiary (Torstveit, 2023). Primary prevention consists of providing and disseminating reliable educational resources. Secondary prevention includes early identification of those at risk of developing REDs, together with prompt and correct diagnosis. For example, regardless of whether an athlete or dancer, amenorrhoea in a woman of reproductive age (apart from physiological amenorrhoea of pregnancy) is never “normal”; whether blood tests are in range, or not. The tertiary level of prevention encompasses evidence-based treatments. As mentioned above, NICE guidelines are now in line with Endocrine Society and IOC in advising temporising HRT for bone protection in FHA. Not the COCP which masks underlying hormone dysfunction and is not bone protective. Similarly, thyroxine is not advised where there is downregulation of this axis as a consequence of REDs. This is not the same as the medical condition of a primary underactive thyroid indicated by raised thyroid stimulating hormone (TSH) (Keay, 2022).
Conclusion
Ultimately, we all have a role to play in supporting exercisers, athletes and dancers in avoiding “the REDs card” (Mountjoy, 2023). This involves the extended multidisciplinary team, starting with the individual exerciser, family, friends and coaches. Then bringing in health care professionals from medicine, dietetics and physiotherapy.
Imbalances in behaviours around exercise and nutrition can have potential negative consequences on all aspects of health and performance. On a positive note, exercise, supported with appropriate nutrition, is an excellent way to achieve and maintain optimal physical, mental and social health and support performance. This is applicable for all ages and levels of exercisers from the recreational to the amateur and elite athlete.
References
Burke LM, Ackerman KE, Heikura IAet al. Mapping the complexities of Relative Energy Deficiency in Sport (REDs): development of a physiological model by a subgroup of the International Olympic Committee (IOC) Consensus on REDs British Journal of Sports Medicine 2023;57:1098-1108.
Drinkwater B, Nilson K, Chesnut C. Bone Mineral Content of Amenorrheic and Eumenorrheic Athletes N Engl J Med 1984; 311:277-281 DOI: 10.1056/NEJM198408023110501
Jurov I, Keay N, Hadžić V et al. Relationship between energy availability, energy conservation and cognitive restraint with performance measures in male endurance athletes. J Int Soc Sports Nutr 2021;18:24. doi:10.1186/s12970-021-00419-3
Jurov I, Keay N, Spudić D et al. Inducing low energy availability in trained endurance male athletes results in poorer explosive power. Eur J Appl Physiol 2022;122:503–13. doi:10.1007/s00421-021-04857-4
Keay N, Overseas A, Francis G. Indicators and correlates of low energy availability in male and female dancers BMJ Open Sport & Exercise Medicine 2020;6:e000906. doi: 10.1136/bmjsem-2020-000906
Keay N, Francis G. Infographic. Energy availability: concept, control and consequences in relative energy deficiency in sport (RED-S) British Journal of Sports Medicine 2019;53:1310-1311.
Keay N, Rankin A. Infographic. Relative energy deficiency in sport: an infographic guide
British Journal of Sports Medicine 2019;53:1307-1309.
Keay N, Francis G, Hind K. Low energy availability assessed by a sport-specific questionnaire and clinical interview indicative of bone health, endocrine profile and cycling performance in competitive male cyclists BMJ Open Sport & Exercise Medicine 2018;4:e000424. doi: 10.1136/bmjsem-2018-000424
Keay N, Francis G, Entwistleet al. Clinical evaluation of education relating to nutrition and skeletal loading in competitive male road cyclists at risk of relative energy deficiency in sports (RED-S): 6-month randomised controlled trial BMJ Open Sport & Exercise Medicine 2019;5:e000523. doi: 10.1136/bmjsem-2019-000523
Keay N. The modifiable factors affecting bone mineral accumulation in girls: the paradoxical effect of exercise on bone. Nutrition Bulletin 2000, 25: 219-222. https://doi.org/10.1046/j.1467-3010.2000.00051.x
Keay N, Fogelman I, Blake G. Bone mineral density in professional female dancers.
British Journal of Sports Medicine 1997;31:143-147.
Mountjoy M, Ackerman KE, Bailey Det al. 2023 International Olympic Committee’s (IOC) consensus statement on Relative Energy Deficiency in Sport (REDs) British Journal of Sports Medicine 2023;57:1073-1097.
Mountjoy M, Ackerman KE, Bailey Det al. Avoiding the ‘REDs Card’. We all have a role in the mitigation of REDs in athletes British Journal of Sports Medicine 2023;57:1063-1064.
Pensgaard AM, Sundgot-Borgen J, Edwards Cet al. Intersection of mental health issues and Relative Energy Deficiency in Sport (REDs): a narrative review by a subgroup of the IOC consensus on REDs British Journal of Sports Medicine 2023;57:1127-1135.
Stellingwerff T, Mountjoy M, McCluskey Wet al. Review of the scientific rationale, development and validation of the International Olympic Committee Relative Energy Deficiency in Sport Clinical Assessment Tool: V.2 (IOC REDs CAT2)—by a subgroup of the IOC consensus on REDs British Journal of Sports Medicine 2023;57:1109-1118.
International Olympic Committee relative energy deficiency in sport clinical assessment tool 2 (IOC REDs CAT2) British Journal of Sports Medicine 2023;57:1068-1072.
Shirley M, Longman D, Elliott-Sale K et al. A Life History Perspective on Athletes with Low Energy Availability. Sports Med 2022 52, 1223–1234. https://doi.org/10.1007/s40279-022-01643-w
Todd E, Elliot N, Keay N. Relative energy deficiency in sport (RED-S) British Journal of General Practice 2022; 72 (719): 295-297. DOI: https://doi.org/10.3399/bjgp22X719777
Torstveit M, Ackerman K, Constantini N et al. Primary, secondary and tertiary prevention of Relative Energy Deficiency in Sport (REDs): a narrative review by a subgroup of the IOC consensus on REDs Br J Sports Med 2023;57:1119–1126.
The action of the sun on skin is the most effective way of making vitamin D. However, even walking around outside naked for 5 hours every day during UK winter months is not sufficient to make adequate vitamin D. Therefore, much to the relief of the audience at the recent BASEM Spring conference, this was not a strategy recommended by Dr Roger Wolman.
Vitamin D is a fat soluble steroid hormone. The majority of which is synthesised in the skin when exposed to ultraviolet B in sunlight, with a small contribution from dietary sources: this vitamin D3 molecule is then hydroxylated twice in the liver and then kidney to produce the metabolically active form of vitamin D. This activated steroid hormone binds to vitamin D receptors in various tissues to exert its influence on gene expression in these cells. The mono hydroxylated form of vitamin D is measured in the serum, as this has a long half life.
Does it matter having low levels of circulating vitamin D during winter months? What are the solutions if moving to warmer climates during the winter is (unfortunately) not feasible? What are the other hormones interact with vitamin D?
What are the beneficial effects of vitamin D, particularly in the athletic population?
Bone
Rickets and osteomalacia are conditions where vitamin D deficiency results in bone deformities and radiographic appearances are characterised by Looser zones, which in some ways are similar in appearance to stress fractures.
In a large prospective study of physically active adolescent girls, stress fracture incidence was found to have an inverse relationship with serum vitamin D concentrations. In adult female Navy recruits monitored during an 8 week training programme, those on vitamin D supplementation had a 20% reduction in stress fracture. However, oestrogen status was a more powerful risk factor at 91% in those recruits reporting amenorrhoea. Vitamin D is, itself, is a steroid hormone with range of systemic effects. As will be discussed below, its interaction with the sex steroid oestrogen has an important effect on bone turnover.
Immunity
Although sanatoriums, for those suffering with tuberculosis, were based on providing patients with fresh air, any beneficial effect was probably more due to vitamin D levels being boosted by exposure to sunlight. Certainly there are studies demonstrating the inhibitory effect of vitamin D on on slow growing mycobacteria, responsible for TB. What about the influence of vitamin D on other types of infection? In a recent publication, evidence was presented that supplementation with vitamin D prevented acute respiratory tract infections. This effect was marked in those with pre-existing low levels of vitamin D. In a study of athletes a concentration of 95 nmol/L was noted at the cut off point associated with more or less than one episode of illness. In another randomised controlled study of athletes, those supplemented with 5,000IU per day of vitamin D3 during winter displayed higher levels of serum vitamin D and had increased secretion of salivary IgA, which could improve immunity to respiratory infections.
Muscle
There is evidence that supplementing vitamin D3 at 4,000IU per day has a positive effect on skeletal muscle recovery in terms of repair and remodelling following a bout of eccentric exercise. In the longer term, dancers supplemented with 2,000IU over 4 months reported not only reduction in soft tissue injury, but an increase in quadriceps isometric strength of 18% and an increase of 7% in vertical jump height.
Synergistic actions of steroid hormones
No hormone can be considered in isolation. This is true for the network interaction effects between the steroid hormones vitamin D and oestrogen. In a study of professional dancers, there was found to be significant differences in serum vitamin D concentrations in dancers from winter to summer and associated reciprocal relationship with parathyroid hormone (PTH). In situations of vitamin D deficiency this can invoke secondary hypoparathyroidism. Although low levels of vitamin D were observed in the dancers, this was not a level to produce this condition. However, there was an increase in soft tissue injury during the winter months that could, in part, be linked to low vitamin D levels impacting muscle strength.
The novel finding of this study was that female dancers on the combined oral contraceptive pill (OCP) showed significant differences, relative to their eumenorrhoeic counterparts not on the OCP, in terms of higher levels of vitamin D and associated reductions of bone resorption markers and PTH. The potential mechanism could be the induction by the OCP of liver enzymes to increase binding proteins that alter the proportion of bound/bioactive vitamin D.
This interaction between steroid hormones oestrogen and vitamin D could be particularly significant in those in low oestrogen states such as postmenpoausal women and premenarchal girls. Menarche can be delayed in athletes, so is there a case for vitamin D supplementation in young non-menstruating athletes? What is the situation for men? Do testosterone and vitamin D have similar interactions and therefore implications for male athletes with RED-S, where testosterone can be low?
Vitamin D is not simply a vitamin. It is a steroid hormone with multi-system effects and interactions with other steroid hormones, such as sex steroids, which are of particular relevance to athletes.
There has been much recent coverage regarding female runners suffering with health and performance issues due to relative energy deficiency in sports (RED-S). What about male athletes? A recent article about male cyclists who explained how they developed RED-S, did not receive as sympathetic a response as articles concerning female athletes. Yet multiple Endocrine network disruption in RED-S, associated with suboptimal health and performance, is equally applicable to male and female athletes.
Although competitive road cycling is excellent for cardiovascular (CV) fitness, why are male cyclists at particular risk of impaired bone health and RED-S? Cycling is a non-weight bearing type of exercise, as is swimming, so does not provide much osteogenic (bone building) stimulus. The additional element in road cycling is that, in the short term, low body weight, with associated low body fat, confers a performance advantage. However this can lead to restrictive nutrition and RED-S, that have adverse effects on health and performance, over the longer term.
A recent study looking at bone acquisition in adolescent males found that bone mass, microarchitecture and makers of bone formation were more favourable in footballers compared with cyclists and swimmers. Swimmers had the lowest Vitamin D, presumably as this is generally an indoor sport (unless you live in Australia where outdoor 50m pools abound). Another study found reduction in femoral neck bone mineral accumulation in adolescent male cyclists compared against increases over the same time frame seen in controls.
What about adult male road cyclists? When runners and cyclists were matched for age and body weight, there were no significant differences in hormone or nutrition status, yet cyclists were 7 times more likely to have osteopenia of the lumbar spine than runners. Similar results were found in another study where competitive male road cyclists were found to have reduced lumbar spine bone mineral density (BMD) for age, despite normal levels of testosterone and insulin-like growth factor 1 (IGF1), although intriguingly an inverse correlation with lumbar spine BMD and IGF1 was found. It appears that the biomechanical stress patterns on the spine in cycling are not oesteogenic in nature, which contrasts with rowing where, although also seated, the biomechanical load exerted through the spine does provide an osteogenic effect.
In addition to the non-load bearing nature of cycling on the skeleton, restrictive nutrition can contribute to suboptimal bone health. Reducing energy availability by restricting energy intake whilst increasing training load can be a strategy, especially during pre-season training to reduce body weight and body fat. Essentially, cycling up a steep incline demands less power through the pedals if your body weight is low. Nevertheless, reducing energy availability runs the risk of developing RED-S, associated Endocrine dysfunction and suboptimal bone health, on top of the non-beneficial mechanical osteogenic effect of cycling. On a practical note, with long training rides in the saddle it can be physically and practically difficult to fuel optimally. Recent research in female athletes shows that within day energy deficits magnify hormonal disruption. Could this be a factor in male cyclists where consistent fuelling is either actively avoided and/or practically difficult?
The psychological element of disordered eating has been described amongst elite male cyclists. Male cyclists, in particular, collect many metrics associated with training and racing which could be a manifestation of a drive to perfectionism. Determination and attention to detail are laudable qualities for athletes, but there is a fine line when the balance swings to behaviours and attitudes that can be detrimental to health and performance. Even starting off with good intentions can lead to problems as seen with the growing emergence of orthorexia: “clean eating”, which, ironically, becomes detrimental to health and performance with exclusion of food groups such as carbohydrates.
Exclusively practising a non weight bearing sport such as cycling although great for CV fitness, is not so good for bone health. Does this matter? Potentially injury is more likely in bike spills, which occur both in training and competition even for the most experienced bike handler. Combined with the drive for low body weight in competitive road cycling, health and performance issues can be compounded with RED-S. What are the solutions for the cyclist to support favourable body composition and bone health, which ultimately also optimises performance? A further planned study, following a current pilot study of competitive road cyclists, aims to investigate the potential beneficial effects of strength and conditioning to load the skeleton combined with a review of nutrition. See details of next study to see if you wish to participate.
Unfortunately I continue to see athletes, both male and female, whose health and athletic performance is hampered due to Relative Energy Deficiency in Sports (RED-S). There have been some high profile athletes who have been very open about how RED-S has affected them, alerting younger athletes to potential pitfalls.
Does this issue warrant highlighting? Yes! The athletes I see and those that speak out are only just the tip of the iceberg. In a study of exercising females, half were found to have subtle menstrual hormone disruption such as luteal phase deficit or anovulation. A third were amenorrhoeic, with no periods at all. All women of reproductive age, whether an athlete or not, should have regular periods, otherwise there are potential serious health and performance sequaelae. However studies in both the USA and Australia have revealed that the majority of young exercising women are not aware of the link between menstrual disruption and deleterious, potentially irreversible effects on bone health.
The impact of non-integrated periodisation of training, nutrition and recovery has evolved since the early description of the female athlete triad. The constellation of amenorrhoea, disordered eating and osteoporosis is now considered to be a clinical spectrum. In turn the female athlete triad is part of a much broader picture of RED-S, which includes adverse multi-system effects beyond bone health and is also seen in male athletes.
Although an athlete may appear healthy, what are the underlying Endocrine disruptions occurring in RED-S that ultimately will impede both optimal health and performance to full potential? In general, female exercisers are more susceptible to internal and external perturbations as the female Endocrine system is more finely balanced than in males. Nevertheless, in a study of male athletes, in the short time period after completing a training session, bone turnover was adversely affected, with an increase in markers of resorption relative to formation, if an athlete did not refuel rapidly with protein and carbohydrate. In the now classic research by Loucks, 5 days of manipulated energy restricted availability, via dietary intake and exercise output, caused disruption in LH pulsatility in previously eumenorrhoeic women. From this research and subsequent studies, not only is the reproductive axis disrupted with reduced energy availability, in addition hypothalamus-pituitary-thyroid (decreased T3) and adrenal axes (increased cortisol) and decreased IGF1 due to relative GH resistance are all disrupted. These interactive hormonal dysfunctions occur even before reduction in sex steroids. A recent study demonstrated that beyond the average energy availability over a 24 hour time window, within day energy deficits in terms of duration and magnitude are associated with a greater degree of disruption of Endocrine and metabolic markers, in particular decreased oestradiol and increased cortisol. So consistency of nutrition, not only during a training season but from day to day is vital.
Although energy availability is the crucial factor in the pathophysiology of RED-S, measuring this is not practical for all athletes in terms of accuracy and cost. Clinical menstrual status in female athletes and basic Endocrine markers are proposed as being more reliable and accessible. The Endocrine system is very sensitive to internal and external perturbations, as described above, and presages performance consequences of RED-S, such as injury. An important starting point is for all female athletes is to ask themselves: are my periods regular? This is also a vital question that coaches and parents need to consider for athletes in their care. If the answer is no, then this needs to be assessed, ideally by those with experience in Sports Endocrinology.
Why are these clinical and biochemical markers of Endocrine dysfunction important for athletes? Essentially there are significant health and performance implications for athletes. As outlined in the stories of female athletes, by the time career limiting stress fractures become obvious, typically in early twenties, the Endocrine system has been in disarray for a significant time. Long term, irreversible poor bone health and adverse body composition have been established.
In my opinion, emphasis should be placed on the positive outcome of integrating periodised training, nutrition and recovery to support a functional Endocrine system and therefore optimal health and ability to reach full athletic potential. For example for female athletes, competing in sports where low body mass confers a performance advantage, such as ballet, gymnastics and road cycling, finely tuned neuromuscular skills are essential to reach maximal potential and minimise injury risk. Yet these are the athletes most at risk of developing RED-S, with consequential adverse effects on menstrual cycles, endogenous oestrogen secretion and neuromuscular function.
Rather than reading headlines about the concerning health issues amongst athletes, more guidance for athletes and those working with them, on the warning signs and how to combat RED-S are needed so that athletes can reach their full potential and the headlines become about athlete achievements.
If you are interested in any aspects of Sport/Dance, Exercise and Lifestyle Medicine here are some suggestions:
British Association of Sport and Exercise Medicine Spring Conference 22 March 2018 “Health, Hormones and Human Performance” Covering the Endocrine and Metabolic aspects of Sport, Dance, Exercise Science and Medicine. From the elite athlete to the reluctant exerciser. Aimed at all those members of the multidisciplinary team working with athletes/dancers, plus athletes/dancers and their coaches/teachers.
CPD points awarded from Faculty of Sports and Exercise Medicine FSEM
BASES British Association of Sport and Exercise Sciences CPD awarded
Why? The balance and timing of exercise, nutrition and recovery is key to optimising health and all aspects of human performance. Intricate network interactions between the Endocrine system and metabolic signalling pathways drive these positive adaptations. However, non-integration of these lifestyle factors can disrupt signalling feedback pathways and predispose to maladaptation and potentially disease states.
What? Discussion, led by experienced clinicians and researchers will cover:
· Key role of Sports Endocrinology in health and performance
· Effects of exercise modalities on body composition and bone health
· Machine learning in interpreting biochemical & metabolomic patterns
· Endocrine & metabolic markers in assessing health & training status
· Gut metabolism in supporting health and performance
· Exercise as crucial lifestyle factor in pre-existing metabolic dysfunction
Who? This conference is relevant to all members of multidisciplinary teams supporting both reluctant exercisers and elite athletes. Medics, researchers, physiologists, physiotherapists, nutritionists, psychologists, coaches, athletes. All welcome.
Wales Exercise Medicine Symposium by Cardiff Sports & Exercise Medicine Society 27/1/18. This includes Dr Peter Brukner, founder of the Olympic Sports Medicine Park in Melbourne, and an afternoon session discussing the female athlete through the lifespan. CPD points applied for from the Royal College of Physicians, the Faculty of Sports and Exercise Medicine, REPs and the Royal College Of General Practitioners.
Women in Sport and Exercise Conference 2018 13-14 June Organised by The Women in Sport and Exercise Academic Network and attracting British Association of Sport and Exercise Sciences (BASES) CPD points.
It is not a simple question of what, but when we eat, sleep and exercise.
The Endocrine system displays temporal variation in release of hormones. Integrating external lifestyle factors with this internal, intrinsic temporal dimension is crucial for supporting metabolic and Endocrine health.
Amplitude and frequency of hormonal secretion display a variety of temporal patterns:
Diurnal variation, synchronised with external light/dark. Orchestrated by a specific area of the hypothalamus, the neuroendocrine gatekeeper.
Circadian rhythm, roughly 24-25 hours which can vary with season according to duration of release of melatonin from the pineal gland.
Infradian rhythms longer than a day, for example lunar month seen in patterns of hypothalamic-pituitary-ovarian axis hormone release during the menstrual cycle.
Further changes in these temporal release and feedback patterns occur over a longer timescale during the lifespan.
Hormones influence gene expression and hence protein synthesis over varying timescales outlined above. The control system for hormone release is based on interactive feedback loops. The hypothalamus is the neuroendocrine gatekeeper, which integrates external inputs and internal feedback. The net result is to maintain intrinsic biological clocks, whilst orchestrating adaptations to internal perturbations stimulated by external factors such as sleep pattern, nutrition and exercise.
Circadian alignment refers to consistent temporal patterns of sleep, nutrition and physical activity. Circadian misalignment affects sleep-architecture and subsequently disturbs the interaction of metabolic and Endocrine health. This includes gut-peptides, glucose-insulin interaction, substrate oxidation, leptin & ghrelin concentrations and hypothalamic-pituitary-adrenal/gonadal-axes. The main stimuli for growth hormone release are sleep and exercise. Growth hormone is essential for supporting favourable body composition. These integrated patterns of environmental factors may have a more pronounced effect on those with a genetic predisposition or during crucial stages of lifespan. For example curtailed sleep during puberty can impact epigenetic factors such as telomere length and thus may predispose to metabolic disruption in later life. Regarding activity levels, there are strong relationships between time spent looking at screens and markers, such as insulin resistance, for risk of developing type 2 diabetes mellitus in children aged 9 to 10 years.
In addition to adverse metabolic effects set in motion by circadian misalignment, bone turnover has also shown to be impacted. Circadian disruption in young men resulted in uncoupling of bone turnover, with decreased formation and unchanged bone resorption as shown by monitoring bone markers. In other words a net negative effect on bone health, which was most pronounced in younger adult males compared with their older counterparts. These examples underline the importance of taking into account changes in endogenous temporal patterns during the lifespan and hence differing responses to external lifestyle changes.
For male and female athletes, integrated periodised training, nutrition and recovery has to be carefully planned over training seasons to support optimal adaptations in Endocrine and metabolic networks to improve performance. Training plans that do not balance these all these elements can result in underperformance, potentially relative energy deficiency in sport and consequences for health in both short and long term.
Part 2 will consider the longer term consequences and interactions of these temporal patterns of lifestyle factors, including seasonal training patterns in male and female athletes, on the intrinsic biochronometry controlling the Endocrine and metabolic networks during lifespan.
Metabolic syndrome comprises a cluster of symptoms including: hypertension, dyslipidaemia, fatty liver disease and type 2 diabetes mellitus (T2DM).
The underlying pathological process is insulin resistance which distorts metabolism. Temporal and mechanistic connections have been described between hyperinsulinaemia, obesity and insulin resistance. Insulin levels rise, potentially stimulated by excess intake of refined carbohydrates and in addition the metabolic actions of insulin are attenuated on target tissues such as the liver, skeletal muscle and adipose tissue. At a cellular level, inflammatory changes play a part in this metabolic dis-regulation. Mitochondrial action in skeletal muscle is impaired, compromising the ability to oxidise fat as a substrate, thus resulting in muscle glycolysis and a consequent rise in blood lactate.
Although much attention has been focused on restricting calories and treating elevated lipids with medication (statins), evidence is now emerging that this does not have the anticipated effect of reducing mortality from cardiovascular disease. In addition, it has been proposed that the gut microbiota plays a pivotal role in metabolism, inflammation and immunity.
Metabolic syndrome usually conjures an image of an overweight person with or on the verge of developing T2DM. However there is an interesting group of slim people who are also are at risk of developing metabolic syndrome due to insulin resistance. The majority of women with polycystic ovary syndrome (PCOS) present with menstrual disturbance of some description. However not all display the textbook characteristics of Stein-Leventhal syndrome (overweight, hirsute and with skin problems). There is in fact of spectrum of clinical phenotypes ranging from the overweight to the slim. In all phenotypes of PCOS, the crucial uniting underlying metabolic disturbance is insulin resistance. The degree of insulin resistance has been shown to be related to adverse body composition with increased ratio of whole body fat to lean mass.
Although this confuses the picture somewhat, it also simplifies the approach. In all cases the single most important lifestyle modification is exercise.
Exercise improves metabolic flexibility: the ability to adapt substrate oxidation to substrate availability. Endurance exercise training amongst athletes results in improved fat oxidation and right shift of the lactate tolerance curve. Conversely metabolic inflexibility associated with inactivity is implicated in the development of insulin resistance and metabolic syndrome.
What about nutritional strategies that might improve metabolic flexibility? Ketogenic diets can either be endogenous (carbohydrate restricted intake) or exogenous (ingestion of ketone esters and carbohydrate). Low carbohydrate/high fat diets (terms often used interchangeably with all types of ketogenic diets) have been shown to improve fat oxidation and potentially mitigate cognitive decline in older people.
However, in the case of athletes, the benefits do not necessarily translate to better performance. Despite reports of such diets enhancing fat oxidation and favourable changes in body composition, a recent study demonstrates that this, in isolation, does not translate into improved sport performance. A possible explanation is the oxygen demand of increased oxidation of fat needs to be supported by a higher oxygen supply. The intermediate group of endurance athletes in this study, on the periodised carbohydrate intake, fared better in performance terms. Another recent study confirmed that a ketogenic diet failed to improve the performance of endurance athletes, in spite of improving fat metabolism and body composition. Despite small numbers, this warrants particular mention as the majority of participants were women, who are in general very underrepresented in scientific studies.
In all likelihood, the reason that these type of diets (ketogenic, high fat/low carb: not always well defined!) did not improve sport performance is that only one aspect of metabolism was impacted and quantified. Although fat oxidation, modified via dietary interventions, is certainly an important component of metabolism, the impact on the interactive network effects of the Endocrine system should be evaluated in the broader context of circadian rhythm. For athletes this goes further, to include integrated periodisation of nutrition, training and recovery to optimise performance, throughout the year.
In addition to dietary interventions, medical researchers continue to explore the use of exercise mimetics and metabolic modulators, to address metabolic syndrome. Unfortunately, some have sought their use as a short cut to improved sport performance. Many of these substances appear on the WADA banned list for athletes. However the bottom line is that it is impossible to mimic, either through a dietary or pharmacological intervention, the multi-system, integrated interplay between exercise, metabolism and the Endocrine system.
Only one road to Rome!
Whatever your current level of activity, whether reluctant exerciser or athlete, the path is the same to improve health and performance. This route is exercise, supported with periodised nutrition and recovery. Exercise will automatically set in motion the interactive responses and adaptations of your metabolic and Endocrine systems.
The interactive network effects of the Endocrine system are key in producing effective adaptations to exercise. This in turn results in improved sport performance. Athletes are aware of the crucial role of the Endocrine system in sports performance. Therefore it is not surprising that, on the World Anti-Doping agency (WADA) banned list, the majority of prohibited substances both in and out of competition are hormones, mimetics and hormone and metabolic modulators. In 2013 hormones accounted for 75% of all adverse analytical findings. Use of such substances to enhance performance is not only illegal and against the spirit of sport, but also potentially harmful to the health of the athlete.
Considering some of these prohibited hormones, the usual suspects start with anabolic agents: anabolic androgenic steroids whether these be synthetic derivatives taken exogenously or molecular identical endogenous steroids, including metabolites and isomers, administered exogenously. In a study recently published in the BJSM, female athletes with free testosterone levels in the highest tertile displayed better performance than those in lowest tertile of up to 4.5% in certain power/anaerobic events such as 400m, 800m, hammer and pole jump. This may be due to associated body composition with increased lean mass and “risk taking” behaviour. In 2015, the Court of Arbitration for Sport ruled that the IAAF should suspend the existing upper limit on female athlete testosterone, of 10nmol/l, because at the time there was insufficient evidence that such levels would improve performance in female athletes. In view of the results of this study, the situation may have to be reviewed. This is clearly an ethical dilemma regarding intersex athletes, whose hyerandrogenism is due to endogenous biological factors.
Next up there are peptide hormones/growth factors/mimetics. As previously discussed, growth hormone (GH) proved a challenging peptide hormone for which to develop a dope test. Firstly what are the “normal” ranges for elites athletes, seeing as exercise and sleep are the two major stimuli for GH release? Furthermore, elite athletes represent a subset of the population, for whom the normal range may differ. Secondly exogenous genetically engineered GH is to all intents and purposes identical to endogenous secreted GH, with a relatively short half life. Hence early on in development of a dope test we realised that downstream markers, particularly of bone turnover would have to be used. This brings the discussion to erythropoietin (EPO). In a similar way to GH and allied releasing factors, increases in key surrogate variables producing performance enhancement are measured. In the case of exogenous EPO these are changes in haemoglobin and haematocrit as recorded in an athletes’ biological passport. A recent study on amateur cyclists given EPO in a double blind randomised placebo controlled trial, reported no improvement in a submaximal field test. Although the effects in elite cyclists would arguably be more relevant, this is not possible for obvious ethical reasons. Nevertheless the effects on elite cyclists during maximal efforts, for example in an attack on a mountainous stage in the Tour de France, would not necessarily correlate to amateurs in submaximal conditions, where there may be other limiting factors to performance. In addition athletes may use supraphysiological dosing regimens (“stacking” or “pyramiding”), not necessarily comparable to those used in clinical studies. In my opinion, apart from potential ergogenic benefits, whatever the degree, the intention to “take a short cut” to improve performance is the issue, not to mention the adverse health sequelae, for example, the study noted a thrombotic tendency with EPO, even in modest doses.
Hormone and metabolic modulators have received attention following the fall from grace of Maria Sharapova. Meldonium which is licensed for use in Baltic countries has beneficial anti-ischaemic effects in cardiovascular, neurological and metabolic disease states. Apparently this drug was use amongst Soviet troops during the war in mountainous Afghanistan. Amongst athletes the intended purpose is to improve endurance exercise performance and recovery post exercise. This is an example where an unfortunate spin off from developing drugs to treat disease states, is that such drugs are also see by some athletes as a short cut to enhance sport performance.
Although thyroxine is not on the banned list, there are certainly arguments that exogenous thyroxine should not be given to athletes, unless there is definitive biochemical evidence that the athlete suffers with hypothyroidism: as defined by criteria for diagnosing this condition with consistently elevated thyroid stimulating hormone (TSH) above the normal range, with paired low T4. Thyroid autoantibodies may also provide extra clinical information. The effect of intense training on the hypothalamic-pituitary-thyroid axis is to slightly suppress both TSH and T4, whilst these remain in the normal range. In this instance medicating with exogenous thyroxine would be to support recovery from training, rather than to legitimately treat a proven medical condition. In a similar way a TUE is only justified for testosterone in pathological disorders of the hypothalamo-pituitary-testicular axis and not for suppressed testosterone as a result of training stress.
Unfortunately supplements are a source of preventable anti-doping rule violations (ADRV) representing up to half of the total ADRVs. Either such supplements have not listed all the contents, or contamination has occurred during manufacture. If an athlete wishes to take supplements, certainly it is advisable only to take reliably tested products. Nevertheless even if an athlete unintentionally ingests prohibited substances, then ultimately they are still liable. If claims of the benefits of such supplements sound too good to be true, they probably are. Ultimately supplements will not win races and there is no substitute for periodised training, nutrition and recovery.
Effectively there is an arms race between would-be doper and medical expertise in Sports Endocrinology. However, freezing samples for potential re-analysis with emerging understanding and technology in the future is an added deterrent for athletes whose intention is to take a short cut to improving sport performance.
Health is not just the absence of illness, but rather the optimisation of all components of health: physical, mental and social. Exercise has numerous benefits on all these aspects. However, a recent article in the British Medical Journal described how exercise addiction can have detrimental physical, mental and social effects.
Dedication and determination are valuable qualities required to be successful in life, including achieving sporting prowess. Yet, there is a fine line between dedication and addiction.
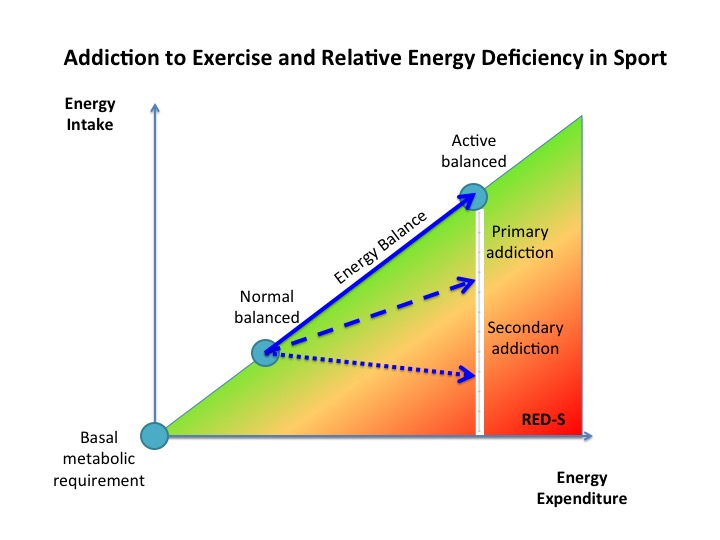
To improve sports performance, cumulative training load has to be increased in a quantified fashion, to produce an overload and hence the desired physiological and Endocrine adaptive responses. Integrated periodisation of training, recovery and nutrition is required to ensure effective adaptation. Sufficient energy availability and quality of nutrition are essential to support health and desired adaptations. On the graph above the solid blue line represents a situation of energy balance, where the demands of increased training load are matched by a corresponding rise in energy availability. This can be challenging in sports where low body weight confers a performance or aesthetic advantage, where the risk of developing relative energy deficiency in sport (RED-S) has implications for Endocrine dysfunction, impacting all aspects of health and sports performance.
Among those participating in high volumes of exercise, what distinguishes a healthy level of commitment from exercise addiction? Physical factors alone are insufficient: all those engaging in high levels of training can experience overuse injuries and disruption in Endocrine, metabolic and immune systems. Equally, in all these exercising individuals, overtraining can result in underperformance.
Psychological factors are the key distinguishing features between the motivated athlete and the exercise addict. In exercise addiction unhealthy motivators and emotional connection to exercise can be identified as risk factors. In exercise addiction the motivation to exercise is driven by the obsession to comply with an exercise schedule, above all else. This can result in negative effects and conflict in social interactions, as well as negative emotional manifestations, such as anxiety and irritability if unable to exercise, including the perceived necessity to exercise even if fatigued or injured.
Two categories of exercise addiction have been described. Primary exercise addiction is the compulsion to follow an excessive training schedule. Without balancing energy intake, the physical consequence may be a relative energy deficiency, as indicated on the graph by the dashed blue line. In secondary exercise addiction, the situation is compounded by a desire specifically to control body weight. These individuals consciously limit energy intake, almost inevitably developing the full clinical syndrome described in RED-S, dragging them down to the position indicated by the dotted blue line on the chart. These situations of exercise addiction can lead to varying risk categories of RED-S.
As described at the start of this blog, there is a blurred boundary between the dedicated athlete and the exercise addict. In practice there is most likely a cross over. For example, an athlete may start with healthy motivators and positive emotional connection to exercise, which can become a primary addiction to adhere rigidly to a training schedule, rather than putting the emphasis on the outcome of such training. In the case of an athlete where low body weight is an advantage, it is easy to appreciate how this could become a secondary exercise addiction, where the motivation for exercising becomes more driven by the desire to control weight, rather than performance.
In order to support those with exercise addiction, discussion needs to focus on adopting a more flexible approach to exercise, by recognising that exercise addiction has detrimental effects on all aspects of current and long term health. Furthermore, in the case of athletes, a multi-disciplinary approach is desirable to help the individual refocus on the primary objective of training: to improve performance. In all situations, discussion should explore modifications to exercise and nutrition, in order to prevent the negative effects of RED-S on health and performance.
Exercise has numerous health benefits and is usually viewed as positive behaviour. However, the outcome of exercise is related to the amount of training, appropriate nutrition and motivation for exercising.