Body Composition for Health and Sports Performance

Focusing on changes in body weight and body mass index (BMI) alone, as outcome measures of lifestyle interventions, ignores the beneficial multi-system and psychological effects of lifestyle medicine, in particular exercise. This includes advantageous changes in body composition for health and performance.
Why is body composition important? Because not all weight is equal in terms of tissue composition and distribution. To support optimal health, favourable levels of lean mass versus fat mass decreases the risk of sarcopenia, associated bone loss and metabolic syndrome. For athletes, high lean mass coupled with low fat mass is related to improved athletic performance, especially in disciplines where strength to weight ratio a major consideration and/or those disciplines such as gymnastics and ballet where an aesthetic component confers a performance advantage.
The range of methods for measuring body composition have advantages and disadvantages in terms of accuracy, accessibility and expense. Although accurate in experienced hands, skin fold measurements are limited to giving a measure of subcutaneous fat. Impedance scales have the advantage of giving a measure of both total and visceral fat percentage, however accuracy is dependent on hydration status, amongst other variable factors. Dual-Energy X-Ray Absorptiometry (DEXA) scan is the “gold standard” for measuring body composition to include bone, lean and fat: both total and visceral. DEXA scan is relatively inexpensive and very low radiation dose compared to traditional X ray or computerised tomography (CT). This method of assessing body composition during training seasons is used by some professional sports teams. The illustration above shows a trained male with total fat in the athletic range. Although simple to measure, BMI does not accurately reflect body composition. All methods of assessing body composition can potentially have role in monitoring changes, for example over training seasons, and trends for individuals rather than relying on the absolute values of metrics measured.
How to go about optimising body composition? Combined exercise and nutritional strategies trigger and reinforce favourable metabolic and Endocrine signalling pathways. The detail of these lifestyle strategies will depend on the clinical context and the objectives of the individual: ranging from a sedentary person trying to improve health and well being, to an athlete aiming to improve sport performance. In all scenarios protein intake is an important factor in supporting lean mass, alongside tailored exercise/training. Temporal considerations for optimising body composition in athletes include the age of the athlete and targeting key competitions during a training cycle and in long term over athletic career. Ultimately optimising body composition has to translate to improved athletic performance for the endurance athlete. So aiming for “high quality weight loss” with retention or even improved lean mass, is more likely to support performance, rather than focusing on fat mass loss in isolation, which may occur in any case as a secondary consequence of integrated periodised training, nutrition and recovery. Striving for weight loss and reduced fat mass without careful monitoring and attention to effects on performance, can run the risk of athletes developing relative energy deficiency in sports (RED-S). Female athletes with functional hypothalamic amenorrhoea have been shown to decreased levels not only of lean and fat mass, but in addition reduced metabolically active brown fat and the associated hormone isirin which promotes fat “browning” and impacts bone mineralisation. In addition, there are differences between male and female athletes to be considered in terms of body composition and cycling performance.
From middle-age, both lean mass and bone mineral density (BMD) decline: sarcopenia and bone health intertwined. In order to mitigate against these changes, resistance exercise is particularly beneficial to stimulate muscle and load the skeleton and for metabolic and cognitive benefits. BMI is particularly misleading as a metric to assess risk of disease in menopausal women. Rather, the finer detail of body composition, for example visceral fat area, is more informative in terms of metabolic and psychological health.
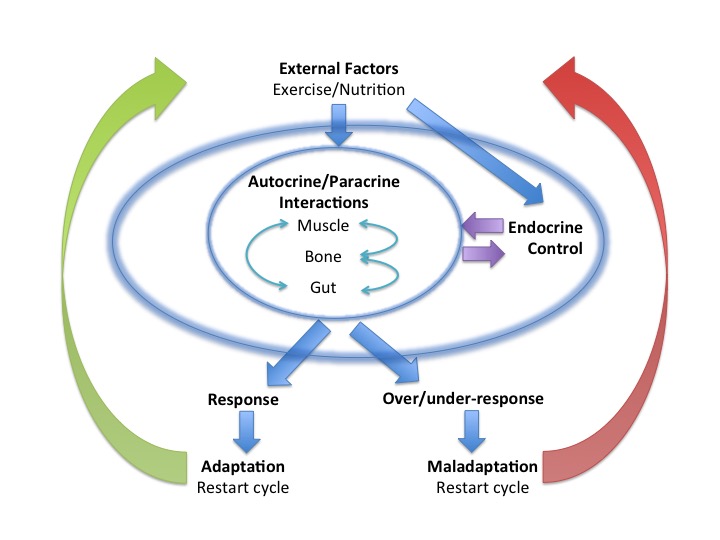
Body composition is a more reliable indicator of health than body weight or BMI. Nevertheless body composition in isolation is not the sole determinant of health and performance. Rather body composition is just one of many multi-system effects mediated by integrated metabolic and Endocrine signalling pathways. These network effects are driven by lifestyle factors including exercise, nutrition and recovery, to determine health and sports performance.
For more discussion and debate on the role of body composition for health and performance BASEM Spring Conference 2018 6 CPD points from FSEM and BJSM approved for international education

References
Challenging those hard to shift, big fat obesity risks BMJ 2017; 359: j5303 British Journal of Medicine 2017
Lifestyle Choices for optimising health: exercise, nutrition, sleep British Journal of Sport Medicine 2107
One road to Rome: Exercise British Journal of Sport Medicine 2107
Current Status of Body Composition Assessment in Sport Review and Position Statement on Behalf of the Ad Hoc Research Working Group on Body Composition Health and Performance, Under the Auspices of the I.O.C.Medical Commission
International society of sports nutrition position stand: diets and body composition Journal of the International Society of Sports Nutrition 2017
Case-Study: Body Composition Periodization in an Olympic-Level Female Middle-Distance Runner Over a 9-Year Career International Journal of Sport Nutrition and Exercise Metabolism 2017
Body composition assessment of English Premier League soccer players: a comparative DXA analysis of first team, U21 and U18 squads Journal of Sports Sciences
Protein Recommendations for Weight Loss in Elite Athletes: A Focus on Body Composition and Performance International Journal of Sport Nutrition and Exercise Metabolism 2017
Optimal Health: For All Athletes! Part 4 – Mechanisms British Association for Sport and Exercise Medicine 2017
Effect of Chronic Athletic Activity on Brown Fat in Young Women Plos One 2106
Kings and Queens of the Mountains Science4Performance
Low bone mineral density in middle-aged women: a red flag for sarcopenia Menopause 2017
Resistance training – an underutilised drug available in everybody’s medicine cabinet BJSM 2017
Benefits of resistance training in physically frail elderly: a systematic review Ageing Clinical and Experimental Research 2017
Is BMI a valid measure of obesity in postmenopausal women? Menopause 2017
Association of visceral fat area with the presence of depressive symptoms in Chinese postmenopausal women with normal glucose tolerance Menopause 2017