Why have my periods stopped?
Periods
Periods, also known as menstruation, are bleeds that occur roughly every lunar month when the lining of the uterus (endometrial lining) is shed. Periods are a result of the fluctuation of menstrual cycle hormones. Oestradiol builds up the endometrial lining and progesterone maintains this. If fertilisation of the egg and implantation of the embryo does not occur, progesterone levels will drop and the endometrial lining will shed. So, periods are a barometer of healthy internal hormone networks. All women of reproductive age, not taking hormonal contraception, and regardless of the amount of exercise undertaken, should experience periods[1].
Eumenorrhea is the name used where a woman is experiencing regular periods, occurring every 22 to 35 days. Polymenorrhoea is where periods occur less that 22 days apart. Oligomenorrhoea is where a woman has less than 9 periods per calendar year. Amenorrhoea is a situation of lack of periods. This can be primary amenorrhoea, where periods have not established by 16 years of age. Or secondary amenorrhoea, where periods have stopped for 6 months or more, in a previously regularly menstruating woman. As regular periods are a sign of healthy internal hormones, women who are not eumenorrheic need to seek answers.
Amenorrhoea is a clinical sign
Amenorrhoea is a clinical sign, not a diagnosis. It is really important to identify the underlying cause of amenorrhoea. Depending on the aetiology of amenorrhoea, oestrogen levels will not necessarily be low. So as a starting point it is essential to establish the cause of amenorrhoea to direct appropriate management.
The figure shows the pathway to follow to identify the cause of amenorrhoea.
Physiological amenorrhoea with high oestradiol In any woman presenting with amenorrhoea, pregnancy, a physiological cause of amenorrhoea, must be excluded. A pregnancy test measures beta human chorionic gonadotrophin (beta hCG) which is secreted by the embryo.
After excluding pregnancy, the cause of amenorrhoea is identified based on follicle stimulating (FSH) and luteinising hormone (LH) levels in keeping with world health organisation (WHO) criteria. Investigations to identify the underlying cause of amenorrhoea are outlined in the updated National Institute for Health and Care Excellence (NICE) in the Clinical Knowledge Summaries (CKS)[2], and summarised in the figure.
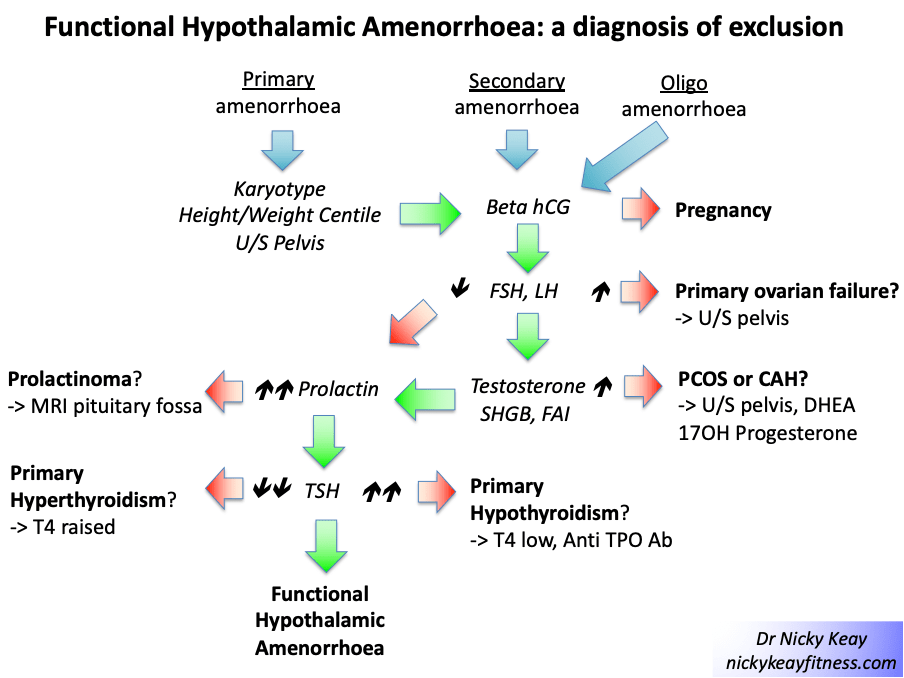
Ovarian causes of amenorrhoea Raised FSH and LH in the presence of low oestrogen suggests primary ovarian insufficiency (POI) in women who are under 40 years of age. The British Menopause Society advise that HRT is more beneficial in improving bone health and cardiovascular markers compared to the combined oral contraceptive pill (COCP) containing ethynyl oestradiol. HRT, unlike the COCP, offers the possibility to deliver body identical oestradiol and progesterone and this optimal form of HRT is available in licensed, regulated forms on the NHS. Barrier methods of contraception are advisable if pregnancy is not sought [3].
Where FSH and LH are not unduly raised and oestrogen is in range, or raised; in the presence of elevated testosterone, this is suggestive of polycystic ovary syndrome (PCOS). Supplementary tests such as dehydroepiandrosterone (DHEA) and 17-hydroxy progesterone
may be considered to exclude congenital adrenal hyperplasia (CAH). In the presence of amenorrhoea, an ultrasound is advisable to check endometrial lining thickness. If this is thickened a “progesterone challenge test” may be considered to induce shedding of the endometrial lining
Hypothalamic-pituitary causes of amenorrhoea Where FSH and LH are low range, together with low range oestradiol, prolactin should be scrutinised to exclude prolactinoma as the cause of hypothalamic amenorrhoea (HA).
Before settling on a diagnosis of functional hypothalamic amenorrhoea (FHA), other endocrine causes of amenorrhea should be considered, such as thyroid disorders. FHA is a diagnosis of exclusion [4].
Functional Hypothalamic Amenorrhea (FHA)
FHA is where amenorrhoea is due to down regulation of the hypothalamic control of menstrual periods. FHA can be a presenting symptom of relative energy deficiency in sport (RED-S) [5]. The good news is that being functional, FHA is a reversible situation. That is not to say that this is an easy situation to reverse. Changes in behaviours around exercise, nutrition and recovery will be needed [6].
The updated NICE guidelines for the management of bone health in the situation of amenorrhoea with low oestrogen advise hormone replacement therapy (HRT) rather than the combined oral contraceptive pill (COCP) [2]. This update is particularly relevant for female exercisers, athlete and dancers presenting with FHA where the underlying cause is RED-S. Pharmaceutical bone protection with transdermal HRT is in keeping with Endocrine Society guidelines [7] and the International Olympic Committee (IOC) consensus statements on RED-S. The British Association of Sports and Exercise Medicine has further information on the website https://health4performance.basem.co.uk/healthcare-professionals/
Conclusions
Amenorrhoea is a symptom, not a diagnosis. It is crucial to identify the underlying cause for amenorrhea in any woman presenting with absent periods. Female hormones are not just about reproduction. These hormones support many aspects of physical and mental health. Oestrogen is the protagonist when it comes to mediating the multisystem beneficial effects on the musculoskeletal, cardiovascular and neurological systems. So, where amenorrhoea is accompanied by low levels of oestrogen it is essential to address the underlying cause and consider providing temporising oestrogen replacement in line with updated NICE guidelines, discussed in previous blog https://nickykeayfitness.com/2022/05/04/female-hormone-health/
References
1 Keay N. What’s so good about Menstrual Cycles? British Journal of Sports Medicine 2019 https://blogs.bmj.com/bjsm/2019/02/08/whats-so-good-about-menstrual-cycles/
2 National Institute for Health and Care Excellence (NICE) Clinical Knowledge Summaries (CKS) Managing risk of osteoporosis (primary and secondary amenorrhoea) 2022 https://cks.nice.org.uk/topics/amenorrhoea/management/secondary-amenorrhoea/#managing-osteoporosis-risk
3 British Menopause Society https://thebms.org.uk/publications/consensus-statements/premature-ovarian-insufficiency/
4 McCarthy O, Pitt J, Keay N et al Passing on the exercise baton: what can endocrine patients learn from elite athletes? Clinical Endocrinology 2022 https://onlinelibrary.wiley.com/doi/10.1111/cen.14683
5 Mountjoy M, Sundgot-Borgen JK, Burke LM, et al IOC consensus statement on relative energy deficiency in sport (RED-S): 2018 update British Journal of Sports Medicine 2018;52:687-697.
6 Keay N. Returning to Sport/Dance restoring Energy Availability in RED-S? British Journal of Sports Medicine 2019 https://blogs.bmj.com/bjsm/2019/03/26/returning-to-sport-dance-restoring-energy-availability-in-red-s/
7 Gordon C, Ackerman K, Berga S et al, Functional Hypothalamic Amenorrhea: An Endocrine Society Clinical Practice Guideline, The Journal of Clinical Endocrinology & Metabolism, 2017, 102 (5): 1413–1439, https://doi.org/10.1210/jc.2017-00131

One thought on “Female Hormone Health part 2”