If you are striving to reach your peak performance, then the PEAQ can help you reach your personal full potential. Click here to get started on the PEAQ
Matching your energy intake to your energy demands helps you reach your personal peak health and exercise performance. On the other hand, failing to meet your energy demands results in low energy availability. This increases your risk of developing relative energy deficiency (REDs) and its adverse health and performance consequences.
People of any age, whatever their level and type of exercise, can be at risk of developing REDs; from elite dancers and athletes to recreational exercisers.
The PEAQ is a mobile Application that will guide you through a series of questions about exercise, physical characteristics, nutrition, hormone function and well-being. It just takes a few minutes.
Your PEAQ report instantly generates a REDs Risk Score and provides valuable insights into your energy status and potential risks, along with guidance. The PEAQ is intended for those 16 years of age and over.
The PEAQ has been developed based on in several published research studies where the questionnaire responses and scores have been correlated with measurements of hormones and bone health in athletes in various sports [1-7] and dancers [8-12]. These questionnaires were cited in the updated International Olympic Committee (IOC) consensus statement on REDs 2013.
Assessment of Relative Energy Deficiency in Sport, Malnutrition Prevalence in Female Endurance Runners by Energy Availability Questionnaire, Bioelectrical Impedance Analysis and Relationship with Ovulation status. Clinical Nutrition Open Science 2025S.
Body composition, malnutrition, and ovulation status as RED-S risk assessors in female endurance athletes, Clinical Nutrition ESPEN 2023, 58 :720-721
Keay N, Craghill E, Francis G Female Football Specific Energy Availability Questionnaire and Menstrual Cycle Hormone Monitoring. Sports Injr Med 2022; 6: 177
Nicolas J, Grafenuer S. Investigating pre-professional dancer health status and preventative health knowledge Front. Nutr. Sec. Sport and Exercise Nutrition. 2023 (10)
Nicola Keay, Martin Lanfear, Gavin Francis. Clinical application of monitoring indicators of female dancer health, including application of artificial intelligence in female hormone networks. Internal Journal of Sports Medicine and Rehabilitation, 2022; 5:24.
Nicola Keay, Martin Lanfear, Gavin Francis. Clinical application of interactive monitoring of indicators of health in professional dancers J Forensic Biomech, 2022, 12 (5) No:1000380
Mountjoy M, Ackerman KE, Bailey DM et al 2023 International Olympic Committee’s (IOC) consensus statement on Relative Energy Deficiency in Sport (REDs) British Journal of Sports Medicine 2023;57:1073-1098
This article explores the current state of play regarding relative energy deficiency in sport (REDs), highlighting the recent updates from the International Olympic Committee (IOC) consensus statement September 2023. Psychological factors and mental health are recognised as having a reciprocal relationship in both the aetiology and outcome of chronic low energy availability leading to REDs. This has important implications in terms of prevention and management of individuals experiencing REDs. Unintentional or intentional unbalanced behaviours around exercise and nutrition leads to a situation of low energy availability. Low energy availability is not synonymous with REDs. Rather cumulative, sustained low energy availability, particularly low carbohydrate availability, leads to the clinical syndrome of REDs comprising a constellation of adverse consequences on all aspects of health and performance. This situation can potentially arise in both biological sexes, all ages and level of exerciser. This is of particular concern for the young aspiring athlete or dancer, where behaviours are being established and in terms of long-term consequences on mental and physical health. The mechanism of sustained low energy availability leading to these negative health outcomes is through the adaptive down regulation of the endocrine networks. Therefore, raising awareness of the risk of REDs and implementing effective prevention and identification strategies is a high priority.
Introduction
Relative energy deficiency in sport (REDs) was first described in the International Olympic Committee (IOC) consensus statement published in the British Journal of Sports and Exercise Medicine (BJSM) 2014(Mountjoy, 2014). Since then, there have been updates published in 2018 (Mountjoy, 2018) and most recently in September 2023 (Mountjoy, 2023).
Seminal studies of female collegiate runners in 1980s found that those athletes with higher weekly training load, but same food intake as those with lower training load, experienced menstrual disruption, including secondary amenorrhoea and poor bone health (Drinkwater, 1984). This led to the description of the female athlete triad, which comprises a clinical spectrum of eating patterns, menstrual function and bone health. This ranges from optimal fuelling, menstrual function and bone health; to eating disorders, amenorrhoea and osteoporosis.
However, with further evidence emerging it became apparent that the impact of under fuelling is not confined to menstrual and bone health. Rather that the consequences of under fuelling are multisystem and can include male athletes. This led to the initial description of REDs in 2014 as a syndrome comprised of the potential adverse effects on many systems in the body with both physical and mental health implications. Crucially, unlike the female athlete trad, REDs also included the potential negative sequalae on athletic performance. Ultimately the goal for all athletes is to perform to their best, so REDs is not something of interest just in academic or clinical circles. REDs is highly relevant to both biological sexes and all levels and ages of exerciser.
What is Energy Availability?
The underlying aetiology of REDs is low energy availability. The life history theory describes how biological processes compete for energy resources (Shirley, 2022). Energy requirement for movement is prioritised from an evolutionary point of view in order to take evasion action from predators. The residual energy from food intake is described as energy availability. This is roughly equivalent to resting metabolic rate for the individual. Simply lying in bed all day, staying alive, is high energy demand for humans as homeotherms. The numerical value of energy availability is expressed in Kcals/Kg of fat free mass. The energy availability requirement for health will vary between individuals depending on sex, age and body composition. Although energy availability is a very useful concept, in practice is it not actually measured outside of the research setting. Rather objective surrogates indicating energy availability can be measured such as triiodothyronine (T3) which is used as a primary indicator of low energy availability as outlined in the update REDs clinical assessment tool described in further detail below (Stellingwerff, 2023 ).
An important highlight from the updated consensus statement on REDs is that it is specifically low carbohydrate availability that is most detrimental, especially for reproductive hormone networks. Comparing isocaloric intake, where there is a low proportion of energy from carbohydrate, this has the most marked negative consequence on both hormone health and performance. The mechanism of sustained low carbohydrate availability appears to involve the hormone leptin, an adipokine, secreted by adipose tissue. Low levels of leptin cause suppression of the reproductive axis via the hypothalamus-pituitary axis (Keay, 2022).
Aetiology of Low Energy Availability
Low energy availability is a situation where, once energy demand from movement has been met, the residual energy available is insufficient to support the functioning of other biological life process.
Low energy availability could arise unintentionally or intentionally (Keay, 2019). Unintentional low energy availability is where an exerciser does not appreciate the energy demands of exercise and other activities with an energy demand. For example, many athletes will not consider the energy required to “commute” to a training session on foot or bike. Unintentional low energy availability could be due to practical issues: for example, a long cycle ride over several hours will require the cyclist to take nutritional sources in the pockets of clothing and/or plan ahead suitable stops where it is possible to obtain nutrition. Similarly, going on a training camp, especially at altitude, will greatly increase energy demand from exercise and needs to factored in. Finances could also be a limiting factor.
On the other hand, intentional low energy availability is where an exerciser intentionally restricts nutrition intake in the belief that this might confer a performance advantage in terms of body weight, composition or shape. This is particularly associated with any exercise against gravity such as running, road cycling, climbing; weight category sports like martial arts and aesthetic forms of sport (diving, gymnastics) and dance.
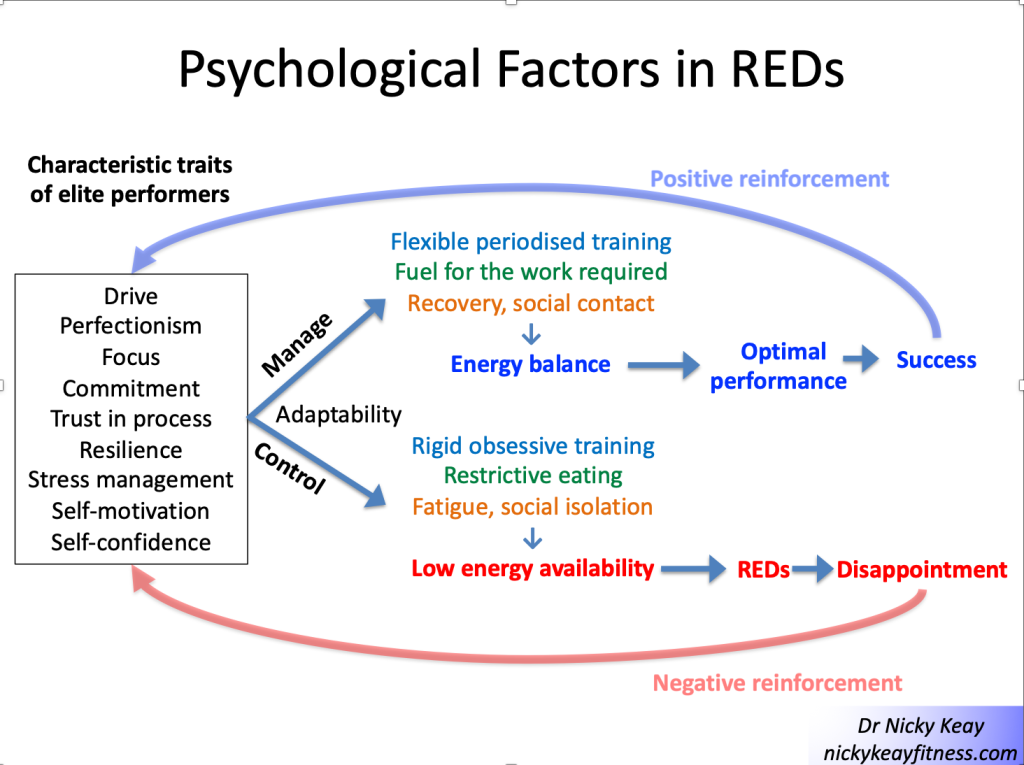
For individuals with intentional low energy availability, psychology and mental health can have a reciprocal interaction (Pensgaard, 2023). Those exercisers with personality characteristics such as self-motivation, perfectionism can be very laudable traits in terms of dedication to exercise training to achieve success. However, when these characterises impact and support rigid behaviours around training and nutrition, this can become problematic. This is shown in Figure 1 “Psychological factors in REDs”. Those who are able to adapt to external pressures and have a flexible approach to training and nutrition are more likely to experience positive outcomes. Whereas those who have a more rigid approach, which might include disordered eating and or an eating disorder and/or exercise dependence are more likely to experience negative outcomes. This reinforces self-doubt and culminates in a vicious circle of perpetuating rigid behaviours and negative outcomes in terms of both physical and mental health.
Evidence for this interaction between psychological factors and risk of REDs was found in our study of dancers, referenced in the updated IOC consensus statement. A significant relationship was found between psychological factors such as anxiety around body shape/weight and missing training. These psychological factors in turn had significant associations between physical manifestations of low energy availability (low body weight) and physiological outcomes (menstrual irregularity) (Keay, 2020). Similarly, in more of our published research papers referenced in the IOC consensus statement focusing on male athletes, an significant association was found between cognitive nutritional restraint and negative physiological and performance outcomes (Jorov, 2021).
This reciprocal interaction between internal and external factors is a systems biology approach, highlighted in the recent updated IOC consensus statement. From a physiological point of view the brain is a high energy demand organ, requiring a good supply of glucose. So low carbohydrate availability will restrict this cerebral supply, which can impair cognitive function and ultimately good decision making. It is interesting to reflect that the neuroendocrine gatekeeper, the hypothalamus keeps a watching brief on internal and external factors, not distinguishing between the source of stressors when putting in motion an adaptive response (Keay, 2022).
Consequences of Low Energy Availabiity
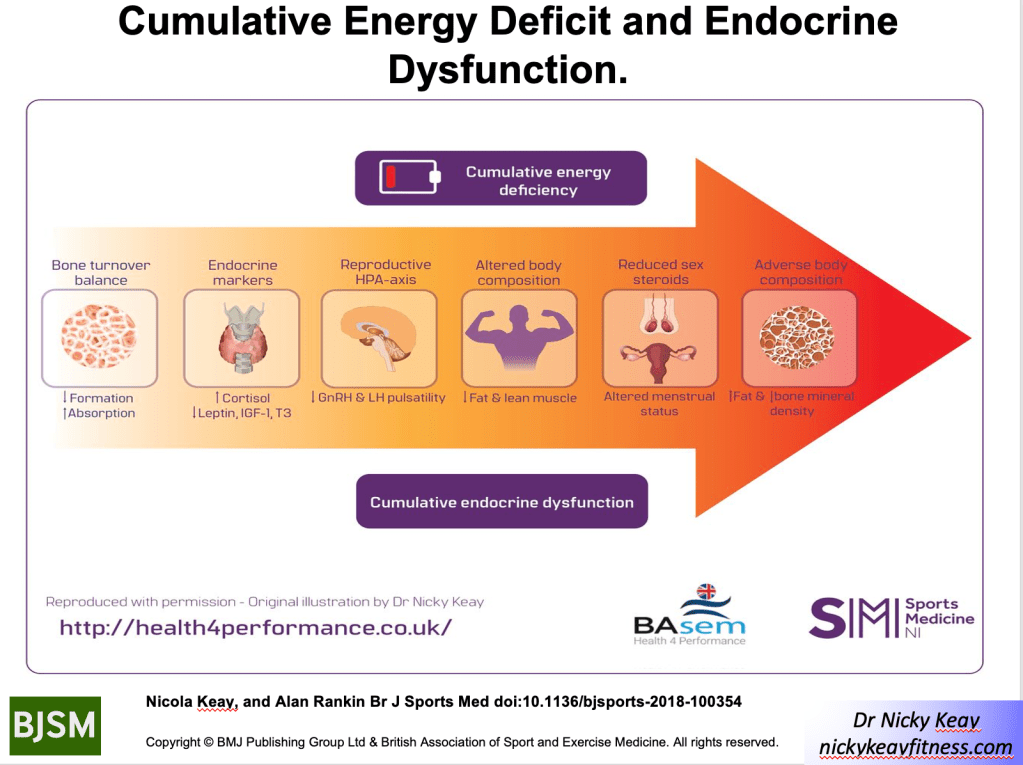
Low energy availability is not synonymous with REDs. Indeed, short term low energy availability might initially bring some good performances. Low energy availability becomes problematic depending on the time scale, which in turn determines the degree of adaptive response, described in the clinical physiological model of REDs (Burke, 2023). The first system to adapt to low energy availability is bone: bone turnover moves in favour of resorption over formation. This is why bone stress responses, specifically bone stress fractures, can be an early warning sign of REDs and designated a primary indicator in the updated IOC consensus statement. There will follow sequential down regulation of metabolic rate mediated via the thyroid axis, followed by the reproductive axis. In women primary amenorrhoea or sustained functional hypothalamic amenorrhoea (FHA) of 6 months or more duration is a severe primary indicator of REDs. In men, low rage testosterone is a severe primary indicator. Ultimately body composition will be adversely affected, with the only endocrine system to be up regulated being that of the hypothalamic-pituitary-adrenal axis (Keay, 2019).
Health
Cumulative low energy availability causes the syndrome of REDs, which produces progressive adverse effects on all aspects of health: physical, mental and social, described in the REDs conceptual model. Poor sleep will compound these negative health effects (Keay, 2022).
Performance
Although there may be some initial good performances, chronic low energy availability will result in adverse performance consequences of REDs, described in the REDs performance conceptual model. In our referenced papers in the consensus statement, we found that in male athletes, short term low energy availability impacted performance (Jurov, 2022). In another of our referenced studies we showed that male cyclists in sustained low energy availability over 6 months, not only experienced bone loss commensurate to astronauts in space, but these cyclists also underperformed compared to their energy replete fellow cyclists (Keay, 2019). On a positive note, explaining to athletes and dancers that improving energy availability will improve their performance, can help in overcoming problematic behaviours.
Identification of those at risk
In view of the potential adverse health and performance effects of REDs, it is a priority to raise awareness of this risk to affect prevention. To this end the British Association of Sports and Exercise Medicine (BASEM) has a website health4performance.co.uk dedicated to providing reliable information on REDs for athletes, parents, coaches and health care professionals together with BASEM endorsed online courses. Targeting and identifying those at increased risk is very important. Young athletes and dancers can be most severely affected as down regulation of hormone function due to low energy availability can cause delay in growth and development. In particular, delayed puberty and menarche dampens the accrual of peak bone mass, with implications for bone health (Keay, 2000). Furthermore, there is evidence that these adverse effects on bone health might not be fully reversible (Keay, 1997)
From a psychological point of view, the young aspiring athlete and dancer is also at heightened risk. Explored and viewed by many dancers in “The Dark Side of Ballet Schools” Panorama (season 33, episode 28). Selection for specialised training will inevitably favour those who are self-motivated and dedicated. In a group of individuals sharing similar psychological traits this could act as a “breeding ground” for reinforcing these characteristics in ways that could lead to behaviours which are not conducive to positive outcomes. Rather reinforcing the negative interpretation of external and internal factors, leading to a vicious circle of reinforcing attitudes and behaviours leading to REDs, as described in Figure 1
Risk stratification
Early identification of those at risk of developing REDs is an important preventative strategy. Especially for young aspiring athletes and dancers where behaviours around eating and exercise are being developed and established. A step-by-step approach is provided in the updated version 2 of the Relative Energy Deficiency in sport Clinical Assessment Tool (REDsCat v2) to identify and risk stratify individuals (Stellingwerff, 2023 ). Initial, low cost, screening questionnaires can be helpful, particularly if tailored to a specific sport/activity or dance. For example: sports specific energy availability questionnaire (SEAQ) (Keay, 2018) and dance energy availability energy questionnaire (DEAQ) (Keay, 2020). This can be helpful in identifying those individuals where further investigation is clinically indicated. As REDs is a diagnosis of exclusion, targeted blood testing excludes medical conditions per se and provide objective quantification in the stratification of risk. Severe primary indicators of REDs are issues in the reproductive axis: long duration of amenorrhoea in females and low range testosterone in males.
From a combination of all these results the individual can be placed in an appropriate risk category. The updated REDs CAT v2 includes a finer grained approach with four categories from green, yellow, amber to red.
This assessment also provides the background on which to base the appropriate level of support. For all, management will be directed at restoring energy availability and include modification of training and nutritional intake. However, the details will vary according to the severity of REDs. Individuals with intentional REDs, especially when formally diagnosed with an eating disorder, will need most intensive input than a person with transient unintentional low energy availability.
Management
A nuanced approach is required for individual athletes, depending on their risk stratification and biopsychosocial factors. In all cases some degree of psychological support will be helpful. Involvement of the extended multidisciplinary team is ideal: medical doctor, dietician, coach and parent (where appropriate) with the athlete/dancer at the centre.
In order to restore energy availability this will require careful discussion around nutrition in terms of consistency of eating patterns and composition of food groups consumed. This starts with regular meals containing good portions of complex carbohydrate and protein. Studies show that inconsistent intake of carbohydrate (eg “backloading” eating to the evening) produces an unfavourable hormone profile. Fuelling around training is also a high priority for hormone health and driving positive adaptations to exercise. Pre training consumption of carbohydrate together with post training refuelling with both complex carbohydrate and protein within 20 minutes of stopping are important behaviours for favourable hormone response to exercise (Keay, 2022).
In terms of pharmacological intervention, NICE guidelines have been updated 2022 in recommending body identical hormone replacement therapy (HRT) over the combined oral contraceptive pill (COCP) for bone protection in those with evidence of bone poor health due to functional hypothalamic amenorrhoea (FHA) as a consequence of REDs (BASEM, 2023). Poor bone health is defined as age matched Z score < -1 of the lumbar spine (trabecular bone particularly sensitive to low oestradiol) and/or 2 or more stress fractures at a site of concern (trabecular rich bone). For male athletes/dancers external testosterone is not appropriate as this supresses internal hormone production. Furthermore, testosterone is on the world anti-doping authority (WADA) banned list and it is not possible to obtain a therapeutic use exemption (TUE) as REDs is a functional condition, not a medical condition.
Prevention
Prevention is always the ultimate goal. In order to achieve this aim, a cultural shift in sport and dance is required. Emphasis on the fact that health is a prerequisite for performance. Pursuing a lighter body weight or leaner body composition will not automatically lead to improved performance. Each individual will have a personal tipping point. As we are all different, there is no such thing as a generic “ideal” weight/shape/body composition.
In practical terms, prevention can be considered as primary, secondary and tertiary (Torstveit, 2023). Primary prevention consists of providing and disseminating reliable educational resources. Secondary prevention includes early identification of those at risk of developing REDs, together with prompt and correct diagnosis. For example, regardless of whether an athlete or dancer, amenorrhoea in a woman of reproductive age (apart from physiological amenorrhoea of pregnancy) is never “normal”; whether blood tests are in range, or not. The tertiary level of prevention encompasses evidence-based treatments. As mentioned above, NICE guidelines are now in line with Endocrine Society and IOC in advising temporising HRT for bone protection in FHA. Not the COCP which masks underlying hormone dysfunction and is not bone protective. Similarly, thyroxine is not advised where there is downregulation of this axis as a consequence of REDs. This is not the same as the medical condition of a primary underactive thyroid indicated by raised thyroid stimulating hormone (TSH) (Keay, 2022).
Conclusion
Ultimately, we all have a role to play in supporting exercisers, athletes and dancers in avoiding “the REDs card” (Mountjoy, 2023). This involves the extended multidisciplinary team, starting with the individual exerciser, family, friends and coaches. Then bringing in health care professionals from medicine, dietetics and physiotherapy.
Imbalances in behaviours around exercise and nutrition can have potential negative consequences on all aspects of health and performance. On a positive note, exercise, supported with appropriate nutrition, is an excellent way to achieve and maintain optimal physical, mental and social health and support performance. This is applicable for all ages and levels of exercisers from the recreational to the amateur and elite athlete.
References
Burke LM, Ackerman KE, Heikura IAet al. Mapping the complexities of Relative Energy Deficiency in Sport (REDs): development of a physiological model by a subgroup of the International Olympic Committee (IOC) Consensus on REDs British Journal of Sports Medicine 2023;57:1098-1108.
Drinkwater B, Nilson K, Chesnut C. Bone Mineral Content of Amenorrheic and Eumenorrheic Athletes N Engl J Med 1984; 311:277-281 DOI: 10.1056/NEJM198408023110501
Jurov I, Keay N, Hadžić V et al. Relationship between energy availability, energy conservation and cognitive restraint with performance measures in male endurance athletes. J Int Soc Sports Nutr 2021;18:24. doi:10.1186/s12970-021-00419-3
Jurov I, Keay N, Spudić D et al. Inducing low energy availability in trained endurance male athletes results in poorer explosive power. Eur J Appl Physiol 2022;122:503–13. doi:10.1007/s00421-021-04857-4
Keay N, Overseas A, Francis G. Indicators and correlates of low energy availability in male and female dancers BMJ Open Sport & Exercise Medicine 2020;6:e000906. doi: 10.1136/bmjsem-2020-000906
Keay N, Francis G. Infographic. Energy availability: concept, control and consequences in relative energy deficiency in sport (RED-S) British Journal of Sports Medicine 2019;53:1310-1311.
Keay N, Rankin A. Infographic. Relative energy deficiency in sport: an infographic guide
British Journal of Sports Medicine 2019;53:1307-1309.
Keay N, Francis G, Hind K. Low energy availability assessed by a sport-specific questionnaire and clinical interview indicative of bone health, endocrine profile and cycling performance in competitive male cyclists BMJ Open Sport & Exercise Medicine 2018;4:e000424. doi: 10.1136/bmjsem-2018-000424
Keay N, Francis G, Entwistleet al. Clinical evaluation of education relating to nutrition and skeletal loading in competitive male road cyclists at risk of relative energy deficiency in sports (RED-S): 6-month randomised controlled trial BMJ Open Sport & Exercise Medicine 2019;5:e000523. doi: 10.1136/bmjsem-2019-000523
Keay N. The modifiable factors affecting bone mineral accumulation in girls: the paradoxical effect of exercise on bone. Nutrition Bulletin 2000, 25: 219-222. https://doi.org/10.1046/j.1467-3010.2000.00051.x
Keay N, Fogelman I, Blake G. Bone mineral density in professional female dancers.
British Journal of Sports Medicine 1997;31:143-147.
Mountjoy M, Ackerman KE, Bailey Det al. 2023 International Olympic Committee’s (IOC) consensus statement on Relative Energy Deficiency in Sport (REDs) British Journal of Sports Medicine 2023;57:1073-1097.
Mountjoy M, Ackerman KE, Bailey Det al. Avoiding the ‘REDs Card’. We all have a role in the mitigation of REDs in athletes British Journal of Sports Medicine 2023;57:1063-1064.
Pensgaard AM, Sundgot-Borgen J, Edwards Cet al. Intersection of mental health issues and Relative Energy Deficiency in Sport (REDs): a narrative review by a subgroup of the IOC consensus on REDs British Journal of Sports Medicine 2023;57:1127-1135.
Stellingwerff T, Mountjoy M, McCluskey Wet al. Review of the scientific rationale, development and validation of the International Olympic Committee Relative Energy Deficiency in Sport Clinical Assessment Tool: V.2 (IOC REDs CAT2)—by a subgroup of the IOC consensus on REDs British Journal of Sports Medicine 2023;57:1109-1118.
International Olympic Committee relative energy deficiency in sport clinical assessment tool 2 (IOC REDs CAT2) British Journal of Sports Medicine 2023;57:1068-1072.
Shirley M, Longman D, Elliott-Sale K et al. A Life History Perspective on Athletes with Low Energy Availability. Sports Med 2022 52, 1223–1234. https://doi.org/10.1007/s40279-022-01643-w
Todd E, Elliot N, Keay N. Relative energy deficiency in sport (RED-S) British Journal of General Practice 2022; 72 (719): 295-297. DOI: https://doi.org/10.3399/bjgp22X719777
Torstveit M, Ackerman K, Constantini N et al. Primary, secondary and tertiary prevention of Relative Energy Deficiency in Sport (REDs): a narrative review by a subgroup of the IOC consensus on REDs Br J Sports Med 2023;57:1119–1126.
Long-term low energy availability leads to adaptive changes throughout the body resulting in the clinical outcomes of REDs
Earlier this week the updated consensus statement from the International Olympic Committee (IOC) on relative energy deficiency in sport (REDs) 2023 was published in the British Journal of Sport Medicine (BJSM)[1]. What are the key points from the range of papers presented in this issue dedicated to REDs?
What’s in a name change?
Making “s” lower case is helpful as relative energy deficiency is not limited to those involved in sport. You can still be at risk of REDs even if you would not consider yourself an athlete; rather “just” someone that does regular exercise. Furthermore, most genres of dance are not sport, yet dancers are another group who can be at risk.
Time scale of low energy availability
The type of adaptive responses to low energy availability is dependent on the temporal component of this energy deficient. Energy availability is the amount of energy “available” once demand from exercise has been accounted for. If this available energy is not sufficient to maintain all the “housekeeping” physiological processes, then the body will respond by going into “eco” mode and down regulating body systems[2]. A small, short-term energy deficit may not be problematic. We have all been in situations where eating patterns don’t go according to plan. For example, a particularly busy time at work, disruption to travel plans, or lack of food availability.
However, sustained, cumulative energy deficit can lead to progressive adaptation shown in the figure.
These adaptive changes across many body systems have adverse outcomes on both health and performance. This is REDs. The clinical syndrome of health and performance consequences of long-term low energy availability. This is what happened in our study of male cyclists referenced in the BJSM publication. We quantified the negative effects of low energy availability on hormone networks, bone health and performance in male cyclists[3]. Those cyclists in low energy availability lost bone mass commensurate with an astronaut in space for 6 months and underperformed in races[4]. This negative impact of low energy availability on performance was underlined in our other studies of male athletes, referenced in the IOC papers [5,6]. Ultimately these are particularly important findings for athletes and their coaches, where performance is the priority.
Menstrual cycles
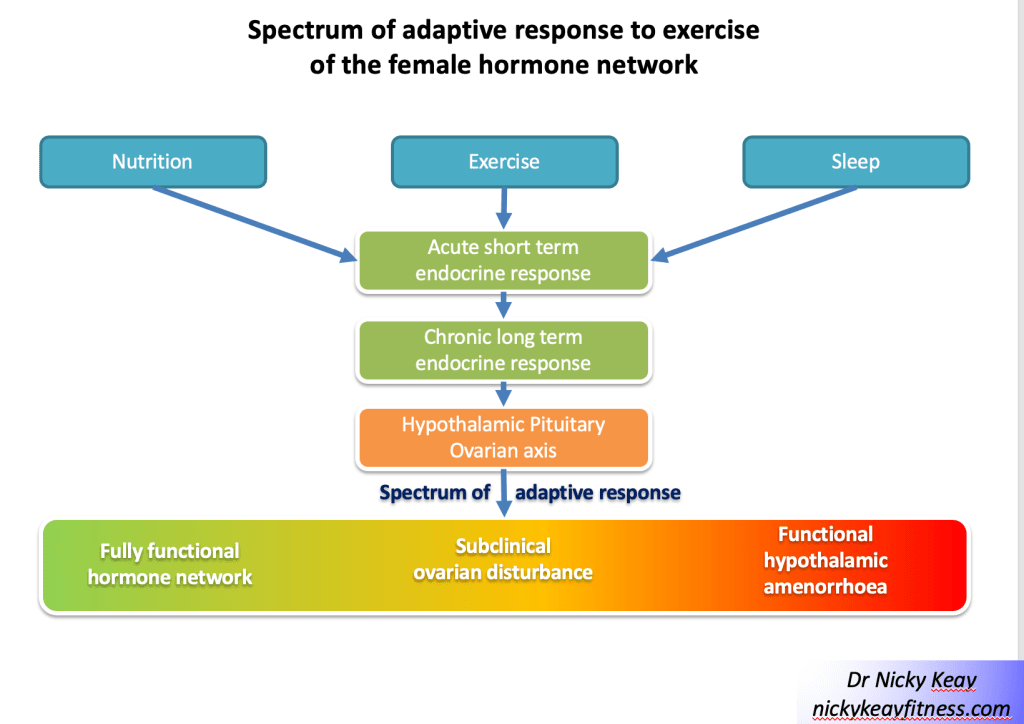
This concept of a gradated adaptive response to the combined effects of training load, nutrition and recovery can be applied when considering the spectrum of reproductive axis responses in female athletes and dancers, ranging from eumenorrhoea, subclinical ovulatory disturbances to functional hypothalamic amenorrhoea[7] shown in figure of Subclinical Ovulatory Disturbance. Functional hypothalamic amenorrhoea (FHA) is potentially just the tip of the iceberg when it comes to adaptive change to low energy availability. Report of menstruation and even signs of ovulation, may belie suboptimal production of progesterone. As progesterone increases metabolic rate, low production could be considered an early response to low energy availability. This hypothesis is currently being tested in a study of dancers, funded by the British Association of Sport and exercise Medicine.
Carbohydrate availability
Although we talk about low energy availability, the updated IOC consensus statement highlights that carbohydrate availability is the key. This is based on evidence that carbohydrate is the main substrate for exercise above a certain intensity. Furthermore, the hormones of the reproductive axis are particularly sensitive to carbohydrate availability. The IOC statement highlights studies, where despite isocaloric diets, those low in carbohydrate resulted in hormone disruption and poorer athletic performance outlined in the statement.
Health is essential for performance
Another important theme is that optimal health is a prerequisite for performance. This includes both physical and mental aspects of health. Many of the psychological characteristics of athletes and dancers can predispose individuals to developing REDs. For example, although dedication, perfectionism and motivation are laudable qualities, these can spill over into behaviours around training and nutrition. This can be associated with exercise dependence and disordered eating patterns.
If an individual is anxious about body shape, weight and food, this can have a negative health outcome. For example, in our study of dancers[8], quoted as a reference in the updated IOC statement, we found that there were significant relationships between anxiety about controlling weight and eating and missing training, and physical outcomes of low BMI and physiological health in terms of lack of regular menstrual cycles. Regular menstrual cycles in women are a barometer of internal healthy hormones. Similarly in another referenced study, we found that cognitive restraint in male athletes had an adverse effect on hormone profiles[9]. How you think impacts hormone health. This interaction is shown by the reversible arrow between psychological factors as both a driver and result of REDs shown in the updated REDs health conceptual model.
Weighty matter
Weight is a measurement of gravity, not athletic potential. Being a certain weight or body composition does not guarantee athletic success. This fact was emphasised by the lead author of the special edition on REDs on the BJSM podcast. Realistically most types of exercise will involve overcoming gravity, nevertheless, there comes a tipping point where being too light weight and/or having too low body fat means being unhealthy and compromising both physical and mental performance. Furthermore, we are all individuals so our personal optimal weight and body composition will be personal to each of us. Not the generic “lighter is faster”.
Identification
Ultimately low energy availability is a concept and not measured outside of research settings. Rather, making a diagnosis of REDs is a diagnosis of exclusion. In other words, other potential medical conditions must be excluded. This can be achieved through a process of identifying those at risk with energy availability questionnaires, followed by assessing clinical symptoms and signs: such as growth trajectories in young athletes and menstrual status in female athletes and dancers. Readily available and reliable investigations such as blood tests and DXA scans are outlined. These clinical findings have been presented as primary, severe indicators (hypothalamic reproductive disruption in men and women), primary indicators, secondary indicators and other supportive factors.
When considering hormone tests is really important to emphasise that even if a result is not out of range, where the result lies in the range is crucial. Together with considering hormones as networks providing a pattern that is informative. For example, in correctly identifying subclinical down regulation of the thyroid or reproductive axis[2].
Risk stratification
Each of indicators described in the consensus statement carries a score, so that an individual can be risk stratified. The REDsCAT2 has a finer grained zone compromising of green, yellow, orange and red, replacing the 3 zoned traffic light system.
Clinical management
Ultimately as the underlying aetiology of REDs is low energy availability, then the aim of supporting an individual experiencing REDs is to restore sufficient energy availability through a combination of nutrition and possibility reducing demand from intense training. As this will involve behaviour change, this can be challenging and a multidisciplinary team approach is advised. Highlighted for female athletes experiencing functional hypothalamic amenorrhoea (FHA) and associated poor bone health, that the combined oral contraceptive pill is not advised. Rather for bone protection in the short-term HRT (transdermal oestradiol and cyclic micronised progesterone) is recommended in line with updated NICE guidelines in UK[10].
The risk of low energy availability and REDs in dancers will be dicsuused at the forthcoming British Association of Sports and Exercise Medicine annual conference 6/10/23. https://health4performance.basem.co.uk/
3 Keay N, Francis G, Hind K Low energy availability assessed by a sport-specific questionnaire and clinical interview indicative of bone health, endocrine profile and cycling performance in competitive male cyclists. BMJ Open Sport Exerc Med 2018;4:e000424. doi:10.1136/bmjsem-2018-000424
4 Keay N, Francis G, Entwistle I et al Clinical evaluation of education relating to nutrition and skeletal loading in competitive male road cyclists at risk of relative energy deficiency in sports (RED-S): 6-month randomised controlled trial BMJ Open Sport & Exercise Medicine 2019;5:e000523. doi: 10.1136/bmjsem-2019-000523
5 Jurov I, Keay N, Spudić D et al Inducing low energy availability in trained endurance male athletes results in poorer explosive power. Eur J Appl Physiol 2022;122:503–13. doi:10.1007/s00421-021-04857-4
6 Jurov I, Keay N, Rauter S Reducing energy availability in male endurance athletes: a randomized trial with a three-step energy reduction. Journal of the International Society of Sports Nutrition 2022;19:179–95. doi:10.1080/15502783.2022.2065111
7 Keay N. Interactions of the female hormone network, exercise training and nature of adaptation. ResearchGate. June 2023 DOI: 10.13140/RG.2.2.28787.71204
8 Keay N, Overseas A, Francis G Indicators and correlates of low energy availability in male and female dancers. BMJ Open Sport ExercMed 2020;6:e000906. doi:10.1136/bmjsem-2020-000906
9 Jurov I, Keay N, Hadžić V et al Relationship between energy availability, energy conservation and cognitive restraint with performance measures in male endurance athletes. J Int Soc Sports Nutr 2021;18:24. doi:10.1186/s12970-021-00419-3
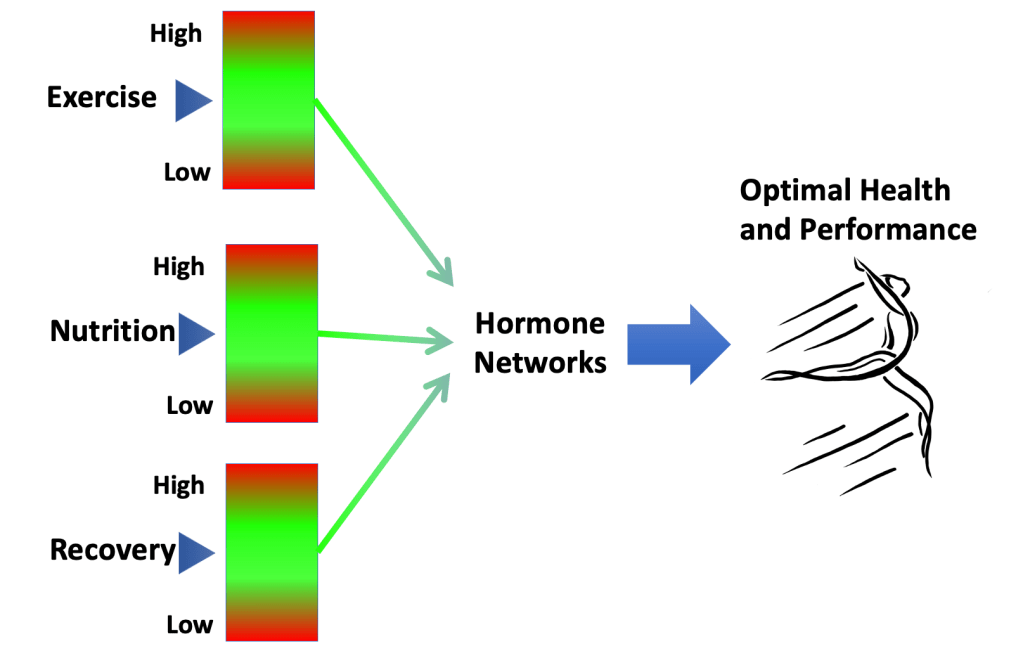
Hormone responses to exercise drive adaptive changes which impact health and performance. The nature of these adaptive changes will depend not only on the exercise training load. There will be individual variation in the nature of the endocrine response.
Given that female hormone networks are one of the most complex of all the endocrine systems, special consideration needs to be given to the exercising female population. Female hormones vary over the menstrual cycle and also change considerably over a woman’s lifespan. So, it is important to consider the detail of endocrine adaptations to exercise in the context of the temporal dimension: both the short term and long term. Furthermore, there will be individual differences in terms of gynaecological age, hormone levels, timings and biological response.
In addition to the effect of exercise training on hormone networks, these endocrine responses will be modulated by other lifestyle factors including the amount and timing of nutrition and recovery. To gain the most effective hormone response to exercise it is important to have an optimal combination of exercise, nutrition and recovery, appropriate for an individual. Any imbalances or mistiming in these external behavioural inputs can potentially lead to suboptimal and even negative hormone adaptations for health and performance.
This narrative opinion piece on exercise endocrinology focuses on the interactive effects of female hormones and exercise over lifespan.
Introduction
Hormones act by determining gene expression. Through this mechanism of action, hormones support homeostasis and are key determinants of all aspects of health. In addition, hormones interact with behaviours, including lifestyle choices around exercise, nutrition and sleep. In this way, hormone networks drive adaptations to exercise. We exercise in the hope and expectation that this will improve our health and fitness, which occurs through the action of hormones in the short term and long term over the lifespan[1].
“If we could give every individual the right amount of nourishment
and exercise, not too little and not too much, we would have found the
safest way to health.”
Hippocrates
Of all the hormone networks, the female hormones of the menstrual cycle are surely the most complex with intricate control mechanisms, including both positive and negative feedback loops. Furthermore, each woman will have individual hormone variations in terms of timing, concentration and biological response to these hormones. This why a personalised approach for each female exerciser is important to support the most beneficial endocrine adaptations to exercise.
Fluctuations in menstrual cycle hormones change over a woman’s lifespan, adding an extra layer of complexity in striving to optimise the interaction between exercise and internal hormones. Furthermore, exercise as a behaviour and lifestyle choice cannot be considered in isolation. Nutrition and sleep are other factors that interact with hormone networks. This triad of exercise, nutrition and sleep act in combination to determine endocrine adaptive responses[1].
This narrative opinion piece will explore the interactions of female hormone networks and exercise over a woman’s lifespan.
Female hormones and exercise interactions over the lifespan
Childhood
During childhood the hypothalamic-pituitary ovarian (HPO) axis is quiescent. This party explains why the energy systems required for anaerobic, intense exercise have not yet developed. For this reason, aerobic type exercise is advised during childhood to match the hormone milieu. Encouraging children to train like adults can lead to mental and physical “burnout”[2]. As girls have an earlier growth spurt than boys, girls are often faster in the 10-12 age group. Although moving into puberty and beyond, the higher levels of testosterone in men account for ergometric differences in exercise performance[3].
Adolescence
The HPO axis comes to life during puberty. The average age of menarche is around 12 years of age, although this may be a bit later in exercising young women. Nevertheless, failure of periods to start by age 15 years, primary amenorrhoea, necessitates medical investigation[4]. If no medical cause is found, a high exercise training load often combined with low energy intake, can be the aetiology of an adaptive down regulation of the HPO axis. This is a health concern as primary amenorrhoea will attenuate the accrual of peak bone mass (PBM), rendering young aspiring athletes at higher risk of bone stress injury with increasing training load when moving from junior to senior ranks[5]. From a study of retired, premenopausal dancers there is evidence that this adaptive down regulation of the reproductive axis can have a long term detrimental effect on bone health[6].
The reproductive years
Regular menstruation acts as barometer of internal hormone health. Menstrual cycle tracking can also help individual women to identify stages in the cycle when certain types of training might lead to the most positive athletic performance adaptations. For example, it has been suggested as beneficial to adaptation to perform strength training during the later follicular phase where oestradiol predominates and more endurance training during the luteal phase of the cycle where progesterone is the dominant ovarian hormone[7]. Nevertheless, the practical challenge is correctly identifying the timing of phases of the cycle associated with these hormone profiles. Although evidence indicates that the main source of temporal variability occurs during the follicular phase[8], even taking this into account there will be individual variation in terms of levels of hormones and biological response to these. Most likely these variations between women account for the finding of a null effect of the menstrual cycle on exercise performance from a large meta-analysis study[9] suggesting that statistical significance is not necessarily synonymous with clinical significance. This means a personalised approach is needed when matching up training and female hormones to gain the maximal positive adaptations for the individual female exerciser.
Functional hypothalamic amenorrhoea
Functional hypothalamic amenorrhoea (FHA) is a lack of periods for 3 months or more where there is no underlying physiological or medical cause. The aetiology of FHA is down regulation at the hypothalamic level due to an imbalance of behaviours around exercise, nutrition, recovery and/or psychological factors. Female exercisers may experience FHA as an adaptive response to low energy availability.
Energy availability is the energy available from food intake, once the energetic demands of exercise have been subtracted. The value is expressed in Kcal/Kg of lean body mass, where sufficient energy availability is roughly equivalent to resting metabolic rate. Low energy availability arises as a result of an imbalance between energy intake and energy demand from exercise training, leaving insufficient energy to maintain health and performance[10]. Chronic low energy availability causes adaptive down regulation of many endocrine axes, including the HPO axis. This leads to the syndrome of relative energy deficiency in sport (RED-S)[11]. In female exercisers, FHA is a clinical symptom of RED-S. FHA is a diagnosis of exclusion and so can be considered an adaptive response to exercise training where low energy availability prevails. From an evolutionary point of view, FHA is an energy conserving mechanism, which allows prioritisation of movement as an escape strategy from danger. However, the global adaptive down regulation of the endocrine system in RED-S has adverse effects on health and athletic performance in the long-term[12]
Although RED-S and overtraining syndrome (OTS) are often described as separate entities, in reality there is no hard dividing line[13]. External factors act in combination to influence hormone networks. Furthermore, the psychological element of how an individual interpretates events, impacts hormone function. In a study of dancers significant correlations were found between psychological factors and the relationship with physical characteristics and the physiological outcome of menstrual status[14]. Non-exercise related stressors were found to cause adaptive, functional neuroendocrine downregulation of the reproductive axis in military recruits participating in arduous training[15]. These findings demonstrate that psychological factors impact endocrine system function, in particular the female reproductive axis. This is why cognitive behavioural therapy (CBT) can help in restoration of full HPO axis function. Psychological factors need to be factored in when considering adaptive responses of the endocrine network to exercise in women.
Subclinical ovulatory disturbances as a spectrum of adaptive endocrine responses
FHA is a very obvious clinical indication of endocrine dysregulation. However, in subclinical ovulatory disturbances, regular periods may belie a down regulatory adaptive response[16]. Subclinical ovulatory disturbances encompass a spectrum of adaptive changes in the HPO axis in response to an imbalance of external inputs around exercise, nutrition and recovery. This is illustrated in Figure 1 Spectrum of adaptive response to exercise of the female hormone network.
The evolutionary purpose of the menstrual cycle is ovulation for reproduction. However, the action of the ovarian hormones associated with the menstrual cycle go far beyond reproduction. Oestradiol is well recognised as vital for many areas of health encompassing the musculoskeletal, cardiovascular, neurological and gastrointestinal systems. Less well recognised is the importance of progesterone, particularly for bone and cardiovascular health[17]. This is why it is crucial to consider the detail of any adaptive changes of the HPO axis to the combinations of exercise training, nutrition and recovery. Furthermore, tracking menstrual cycles alone may not be sufficient as a training metric to assess adaptation to exercise training.
Assessing the details of the menstrual cycle hormone profile would provide insights into the nature and degree of endocrine adaptation of the HPO axis. Although saliva and urine provide convenient mediums from which to measure hormones, these are limited to analysis of steroid hormones in the case of saliva and in urine metabolites for some of the female hormones. The gold standard way of assessing the “full house” of menstrual cycle hormones: follicle-stimulating hormone (FSH), luteinising hormone (LH), oestradiol and progesterone is from a blood sample. Measuring both pituitary and ovarian hormones is important in order to distinguish between hypothalamic and ovarian causes of suspected subclinical ovulatory disturbances. When combined with an exercise specific screening questionnaire and clinical interaction, this approach was found to be effective and well received from female athletes in a longitudinal study of dancers in a professional dance company[18] and in professional female football players[19].
Assessment of menstrual hormone health, using the non-invasive method of Quantitative Basal Temperature (QBT) has been extensively researched and validated[20]. This is based on the principle that progesterone, produced during the luteal phase increases metabolic rate and has a thermogenic effect. However, low levels of progesterone, as found in subclinical ovulatory disturbances, will not be sufficient to produce a sustained increase in body temperature. Low progesterone will prevent an increase in metabolic rate and consequent increased energy intake requirement. Therefore, low progesterone production during the luteal phase, can be considered as an adaptive response to stressors; whether thee stressors arise from high training load, low energy availability or other psychological factors[16].
Further ongoing research will help identify subtle adaptive changes to exercise in the female endocrine system. A validated clinical tool, drawing on a number of inputs, will support the early detection, and monitoring of recovery from, down regulatory adaptive responses of the HPO axis. An example of passing the baton between increasing understanding of the interactions between exercise and the endocrine system[21].
Management of hypothalamic-pituitary-ovarian axis down regulation
Where any degree of adaptive functional endocrine down regulation is detected, the priority is to rebalance the factors of training load, nutrition and recovery to restore full HPO axis function to support optimal health and performance. Psychological support may also be needed to facilitate behavioural change, especially in the case of intentional low energy availability. Depending on the status of bone health in FHA, pharmacological bone protection may be indicated. Although exercise has a positive osteogenic effect on bone, this is negated in the presence of down regulated adaptive endocrine response. The International Olympic Committee (IOC) consensus statement advises treatment with transdermal hormone replacement therapy (HRT) in female exercisers with FHA and 2 or more stress fractures, or a Z score of less than -1 of the lumbar spine[22]. The lumbar spine being trabecular bone is especially sensitive to suboptimal endocrine and nutritional status. The combined oral contraceptive pill (COCP) is not suitable for bone protection as this reinforces down regulation of the HPO axis[23]. Nevertheless, HRT for bone protection is a temporising measure while support is being provided to modify behaviours to ensure health and beneficial endocrine adaptations to exercise.
Intracrinology as a hormone adaptation to exercise?
A novel form of exercise induced hormone adaptation could be attributable to intracrinology. This is the process whereby there is cell specific production of androgens from the precursor DHEA. Androgens produced in this way have a site-specific effect[24]. In answer to the question of whether athletes are born or made, it could be that this intracrine adaptive response could go some way to explaining why higher levels of DHEA, anabolic body composition and performance measures were found on Olympic athletes compared to sedentary controls[25].
Hormonal contraception
It is every woman’s personal choice whether to take hormonal contraception, or not. There are some medical conditions where suppression of ovulation with hormonal contraception can be a helpful management strategy. For example, in the situation of conditions “fuelled” by fluctuation in female hormones such as endometriosis and polycystic ovary syndrome (PCOS). On the other hand, there are situations where hormonal contraception is not appropriate, such as in FHA as outlined above. The jury is still out as to whether hormonal contraception has an effect on endocrine adaptations to exercise and subsequent athlete performance. As with anything to do with female hormones, this is very variable according to the individual. Furthermore, there are such a vast range of hormonal contraceptive preparations, that it is virtually impossible to make generalisations about the impact of hormonal contraception on endocrine adaptation to exercise.
Graduation to menopause
The graduation to menopause marks an important point in a woman’s life when her ovaries stop producing eggs and ovarian hormones. In the face of the changing backdrop of female hormones, the nature of lifestyle factors, including exercise will need to be reconsidered in order to benefit from adaptative changes. Exercise remains the cornerstone and has been shown to help alleviate menopausal symptoms, in particular thermoregulatory issues[26]. Furthermore exercise, with a focus on strength training supports metabolic health[27], body composition[28] and bone strength[29], resisting the consequences of reduced production of sex steroid hormones. HRT can improve quality of life and reduce all-cause mortality, and for many women helps in maintaining their exercise levels[30]. In terms of preparations of HRT, transdermal oestradiol has the optimal profile for metabolic health and body identical oestradiol and micronised progesterone is available in licensed, regulated forms[31]. Testosterone can be given for hypoactive sexual desire disorder (HSDD). Although the aim is to restore testosterone to previous physiological levels, external testosterone cannot be taken by athletes competing in sporting events under world anti-doping authority (WADA) jurisdiction.
Conclusions
The interaction of female hormone function and exercise varies between individuals, resulting in a range of possible adaptive changes, both in the short and long term. As menstrual cycle hormones change over the lifespan, so does the response to exercise. Furthermore, exercise training should not be considered in isolation, rather in combination with other modifiable external factors such as nutrition and recovery. Psychological factors also play a part in determining responses of the female reproductive endocrine axis. It is important to characterise the nature of these endocrine adaptations, as not all will be favourable to health and performance. Therefore, a personalised approach is required when considering the interaction of exercise and female hormones.
[2] Bergeron MF, Mountjoy M, Armstrong N et al. International Olympic Committee consensus statement on youth athletic development. British Journal of Sports Medicine. 2015; 49: 843–851
[3] Hirschberg A. Female hyperandrogenism and elite sport, Endocrine Connections 2020, 9(4), R81-R92.
[4] Gordon CM, Ackerman KE, Berga SL, Kaplan JR, Mastorakos G, Misra M, et al. Functional hypothalamic amenorrhea: An endocrine society clinical practice guideline. J Clin Endocrinol Metab 2017 102(5):1413–39. doi: 10.1210/jc.2017-00131
[5] Ackerman K, Cano S, De Nardo M et al. Fractures in relation to menstrual status and bone parameters in young athletes. Med Sci Sports Exerc. 2015; 47 (8): 1577–1586. https://doi.org /10 .1249 /MSS .0000000000000574
[6] Keay N, Fogelman I, Blake G Bone mineral density in professional female dancers. British Journal of Sports Medicine 1997;31:143-147.
[7] Oosthuyse, T., Strauss, J.A. & Hackney, A.C. Understanding the female athlete: molecular mechanisms underpinning menstrual phase differences in exercise metabolism. Eur J Appl Physiol 2022. https://doi.org/10.1007/s00421-022-05090-3
[8] Fehring RJ, Schneider M, Raviele K. Variability in the phases of the menstrual cycle. J Obstet Gynecol Neonatal Nurs. 2006 ;35(3):376-84. doi: 10.1111/j.1552-6909.2006.00051.x. PMID: 16700687.
[9] McNulty KL, Elliott-Sale KJ, Dolan E et al. The effects of menstrual cycle phase on exercise performance in eumenorrheic women: a systematic review and meta-analysis. Sports Med. 2020; 50: 1813–1827.
[10] Keay N, Francis G Infographic. Energy availability: concept, control and consequences in relative energy deficiency in sport (RED-S) British Journal of Sports Medicine 2019;53:1310-1311.
[11] Mountjoy M, Sundgot-Borgen J, Burke L, Carter S, Constantini N, Lebrun C, et al. The IOC consensus statement: beyond the female athlete triad–relative energy deficiency in sport (RED-S). Br J Sports Med (2014) 48(7):491–7. doi: 10.1136/bjsports-2014-093502
[12] Keay N, Rankin A Infographic. Relative energy deficiency in sport: an infographic guide British Journal of Sports Medicine 2019;53:1307-1309.
[13] Stellingwerff T, Heikura IA, Meeusen R et al. Overtraining Syndrome (OTS) and Relative Energy Deficiency in Sport (RED-S): Shared Pathways, Symptoms and Complexities. Sports Med 2021 51, 2251–2280. https://doi.org/10.1007/s40279-021-01491-0
[14] Keay N, Overseas A, Francis G Indicators and correlates of low energy availability in male and female dancers BMJ Open Sport & Exercise Medicine 2020;6:e000906. doi: 10.1136/bmjsem-2020-000906
[15] Gifford R, O’Leary T, Wardle S etc al. Reproductive and metabolic adaptation to multistressor training in women Endocrinology and Metabolism 2021; 321; 2 https://doi.org/10.1152/ajpendo.00019.2021
[16] Prior, J. C. Adaptive, reversible, hypothalamic reproductive suppression: More than functional hypothalamic amenorrhea. Frontiers in Endocrinology. 2022 Frontiers Media S.A. https://doi.org/10.3389/fendo.2022.893889
[17] Exercise and the Hypothalamus: Ovulatory Adaptations. Prior J. Endocrinology of Physical Activity and Sport 2020. Hackney A., Constantini N. (eds) Contemporary Endocrinology. Humana, Cham. https://doi.org/10.1007/978-3-030-33376-8_8
[18] Keay N, Lanfear M, Francis G. Clinical application of monitoring indicators of female dancer health, including application of artificial intelligence in female hormone networks. Internal Journal of Sports Medicine and Rehabilitation, 2022; 5:24. DOI: 10.28933/ijsmr-2022-04-2205
[19] Keay N, Craghill E, Francis G Female Football Specific Energy Availability Questionnaire and Menstrual Cycle Hormone Monitoring. Sports Injr Med 2022; 6: 177. DOI: 10.29011/2576-9596.100177
[20] Bedford J, Prior J, Hitchcock C et al Detecting evidence of luteal activity by least-squares quantitative basal temperature analysis against urinary progesterone metabolites and the effect of wake-time variability European Journal of Obstetrics & Gynecology and Reproductive Biology 146 (2009) 76–80
[21] McCarthy O, Pitt J, Keay N et al Passing on the exercise baton: What can endocrine patients learn from elite athletes? Clinical Endocrinology 2022: 96(6): 781-792 https://doi.org/10.1111/cen.14683
[22] Mountjoy M, Sundgot-Borgen JK, Burke LM, et al IOC consensus statement on relative energy deficiency : 2018 update British Journal of Sports Medicine 2018;52:687-697.
[24] Labrie F, Martel C, Bélanger A, Pelletier G. Androgens in women are essentially made from DHEA in each peripheral tissue according to intracrinology. J Steroid Biochem Mol Biol. 2017;168:9-18. doi: 10.1016/j.jsbmb.2016.12.007. Epub 2017 Jan 30. PMID: 28153489.
[25] Eklund E, Berglund B, Labrie F, Carlström K, Ekström L, Hirschberg AL Serum androgen profile and physical performance in women Olympic athletes Br J Sports Med 2017; 51(7):1301–1308
[26] Berin E, Hammar M, Lindblom H et al. Resistance training for hot flushes in postmenopausal women: A randomised controlled trial. Maturitas. 2019;126:55-60. doi: 10.1016/j.maturitas.2019.05.005. Epub 2019 May 14. PMID: 31239119.
[27] Bermingham K, Linenberg I, Hall W et al. Menopause is associated with postprandial metabolism, metabolic health and lifestyle: the ZOE PREDICT study. Preprint Lancet. Available at SSRN: https://ssrn .com /abstract 4051462; http://dx .doi .org /10 .2139 /ssrn4051462
[28] Mandrup C, Roland C, Egelund Jon et al. Effects of high-intensity exercise training on adipose tissue mass, glucose uptake and protein content in pre- and post-menopausal women. Frontiers in Sports and Active Living. 2020; (2): 60. https://www .frontiersin .org /article /10 .3389 /fspor .2020 .00060 DOI 10.3389/fspor.2020.00060
[29] Watson S, Weeks B, Weis L et al. High-intensity resistance and impact training improves bone mineral density and physical function in postmenopausal women with osteopenia and osteoporosis: the LIFTMOR randomized controlled trial. JBMR. 2018; 33 (2): 211–220. https://doi .org /10 .1002 /jbmr .3284
[30] Rymer J, Brian K, Regan L. HRT and breast cancer risk. Editorial BMJ. 2019; 367: l5928. https://doi .org /10 .1136 /bmj .l5928
[31] Management of Menopause. Sixth Edition. British Menopause Society 2017
Although relative energy deficiency in sport (RED-S) and overtraining syndrome (OTS) are often described as distinct entities, these can be considered as different facets of the same unbalanced behaviours. For an exerciser these behaviours consist of exercise training load, nutritional intake and recovery.
What is RED-S?
RED-S is a clinical syndrome describing adverse consequences in terms of health and performance due to sustained low energy availability (LEA). LEA is where there is a mismatch between energy intake and the combined energy demand from exercise and resting metabolic rate.
What is OTS?
OTS is a clinical syndrome describing adverse consequences in terms of health and performance when there is sustained non-functional overreaching (NFOR). NFOR is where there is an imbalance between training load relative to recovery.
It’s all about time scales
Thinking about RED-S and OTS in more detail, neither suddenly occur overnight. Rather it is the cumulative effect of energy deficit, or lack of recovery, that causes these syndromes over longer time scales of months.
Short time scales
Facets of LEA and NFOR
For example, the occasional day of suboptimal fuelling/high energy demand, with accompanying relative low energy availability, although not ideal, is nevertheless recoverable. This is shown by the warning masque of LEA of the rotating cube. On the opposite side is the warning masque of NFOR, where there have been some occasions of insufficient recovery over a short time scale of days. As with LEA, this is potentially a recoverable situation.
Longer time scales
Facets of RED-S and OTS
In practical terms, imagine you have been on a training camp or a dance intensive over a week or two. You may have unintentionally incurred a degree of LEA and NFOR, but if you take some time to rest and refuel afterwards, then you will be able to resume usual training fitter and stronger. On the other hand, if you continue to try and train at high intensity, in relative energy deficit you will progress after more weeks and months into the alert red masques of OTS and RED-S. In each case these outcomes are different facets of the same underlying imbalances in athlete/dancer behaviours around training load, nutrition and recovery.
Practical implications
When an athlete or dancer presents with symptoms that could include fatigue, poor sleep, menstrual disruption, recurrent injury (soft tissue or bone), digestive issues and other issues; it is very important to exclude medical conditions. Once this has been done and a diagnosis of exclusion made to confirm a functional issue, then deciding whether to use the terminology RED-S or OTS has a subtle nuance because in practice these syndromes are facets of the same underlying imbalance in athlete behaviours. In all cases the most important aspect is to outline a course of action for the athlete that includes training load, nutrition and recovery, in combination.
Athlete and dancer support
For example, athletes experiencing RED-S often ask if they can restore healthy hormone network function by simply eating more while maintaining a high training load. The simple answer is that this makes recovery less certain as a high training load, specifically high intensity, will most likely mean there is also a degree of NFOR. Therefore, adjustment in all athlete behaviours in synchrony is more effective for health and performance restoration. Similarly in an athlete experiencing OTS, in addition to reduction in training load, optimising nutritional intake will help.
Prevention is always better than cure
The prevention of adverse outcomes for the athlete or dancer is the other important practical implication of considering these clinical syndromes as facets of the same underlying issue. From the rotating cube of unbalanced athlete behaviours, LEA is the precursor to RED-S. Similarly, NFOR is the precursor to OTS. The progression in each case being determined by a longer time scale. Early identification of those at risk is essential to prevent this negative progression. Reversing the situation is a far easier task physiologically and psychological at an early stage of LEA and NFOR, rather than once in a “deeper hole” of RED-S or OTS.
Conclusions
RED-S and OTS being different facets of the same underlying issues of unbalanced athlete behaviours is a concept with practical implications.
References
Keay N. Hormones, Health and Human Potential. 2022 Sequoia books Act 1 Scene 9 “A Balancing Act” and Act 1 Scene 10 “In the Red”.
Presentation from British Association of Sport and Exercise Medicine 23/3/23
Discussion of the interactive effects of exercise in different populations from non-exercisers, those with medical conditions to exercisers, athletes and dancers.
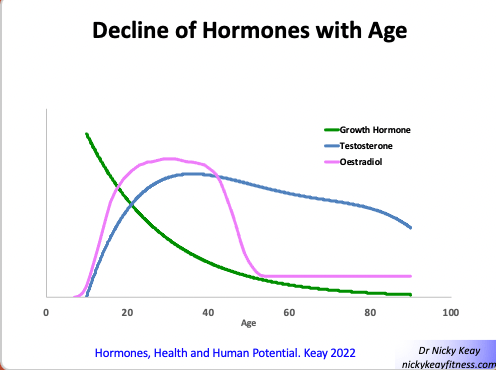
Several hormones decline from middle age onwards. This is a natural physiological process. To keep in step with these hormones changes, this is a good time to review your lifestyle choices.
Hormone changes with age
In both men and women there is a gradual decrease in growth hormone (GH). GH is an anabolic (tissue building) hormone and important for bone health and maintaining a favourable body composition: a good level of muscle mass relative to fat. GH is one of the key hormones driving positive adaptive changes to exercise.
In men there is a slight decline in testosterone from the age of 50 onwards. Testosterone, like GH is an anabolic hormone. In women, the graduation to menopause sees the most dramatic decline in hormone production. Up until menopause the ovaries produce the sex steroid hormones oestradiol (most active form of oestrogen) and progesterone. These play an important role in many areas of health, not limited to reproduction. Oestradiol is queen when it comes to bone and soft tissues like muscles, ligaments and tendons. Cardiovascular health is supported by this dynamic duo of oestradiol and progesterone. The same applies to the neurological system, including cognition and mood. From menopause onwards, the ovaries retire in their production of oestradiol and progesterone. This change in the hormone milieu has an impact in terms of quality of life and long-term health.
How to meet the challenge of hormone changes
There are positive steps in terms of lifestyle choices you can take to mitigate the effects of declining hormones.
Exercise
Exercise remains a cornerstone for hormone and overall physical and mental health. The type of exercise becomes particularly important to mitigate the decline in hormones with age. Strength training will help offset the decline in the anabolic hormones. Several studies show the positive effects of strength training on body composition alongside bone and metabolic health in both men and women. For women navigating perimenopause and menopause, exercise has been shown to help reduce symptoms associated with changing female hormones like hot flushes.
Nutrition
As ever, nutrition including all the food groups and micronutrients is important for hormone health. Protein intake in particularly is important to help resist the tendency to lose muscle mass with declining anabolic hormones. Don’t forget vitamin D, which is actually a steroid hormone that works in synergy with sex steroid hormones. Vitamin D is important for bone, muscle and immune function. Vitamin D is an unusual vitamin in that the main source is not through the diet, rather the action of sunlight on the skin. As sunlight is often in short supply in many countries, supplementation is advisable.
Recovery
You will need more recovery if you are a masters athlete/exerciser. It is when you are resting, especially when asleep that you get fitter. This courtesy of our hormones driving the positive adaptive responses to exercise. The two main stimuli for GH release are exercise and sleep. So making sure you get enough of both these in combination will make the most of your hormones to maintain your health and fitness throughout life.
Next steps for your hormone health
For more insights about the changes in hormones that occur over our lifespan and top tips on practical strategies to maintain health and performance, see my book “Hormones, health and Human Potential”. I also offer presentations and virtual health advisory appointments on all aspects of hormone health to guide individuals of all ages to reach their personal full potential.
At the start of every year there is always a lot of talk about refraining from certain activities like drinking alcohol, advice about eating a particular way, or recommendations to do certain types/amount of exercise. Trends in these lifestyle choices may come and go, but there is one behaviour that remains constant to achieve optimal health. Sleep.
Illustration from “Hormones, Health and Human Potential”
Sleep for hormone health
Why is sleep such an essential component for health? Although being asleep is a physical state of inactivity, it is when many hormone networks are at their most active. For example, one of the main stimuli for growth hormone (GH) release is sleep. Despite its name, GH is not just about growth in children. All adults continue to produce GH and this is an important anabolic (tissue building) hormone. GH maintains a healthy body composition: favouring muscle over fat deposition. GH also plays a role in bone health.
Sleep for fitness
Another stimulus for GH release is exercise. However, you don’t get fitter in real time while you exercise. You get fitter when you are asleep. After stopping exercise and during sleep these two combined stimuli for GH release drive the positive adaptations to exercise. Sleep enables you to become citius, altius, fortius.
Sleep for sex steroid hormone networks
Sleep is also essential for other hormone networks, such as those of the reproductive axis, in both men and women. Studies show that men who have reduced sleep tend to have lower levels of testosterone and poorer bone health. Essentially if you do not have sufficient quality and quantity of sleep this has a negative effect on many aspects of both physical and mental health.
Sleep for metabolic health
Hormones that control appetite and satiety are linked with the sleep/wake cycle. People who have disrupted sleep patterns are more likely to struggle with blood glucose and weight control.
Timing of sleep
The timing of sleep is also important. Hormone networks run on a variety of internal biological clocks, known as biochronometers. The trick is to try and synchronise the timing of your behaviours with these internal biochronometers. If you have an “scheduling conflict” between external and internal clocks, this leads to a situation of circadian misalignment. Circadian misalignment can lead to many adverse consequences on mental and physical health, including metabolic and cardiovascular health. This negative combination can lead to metabolic syndrome which increases the risk of type 2 diabetes mellitus, cardiovascular disease and high blood pressure.
Consequences of disrupted sleep patterns
Shift workers, for example junior doctors, are at risk of developing circadian misalignment. Disrupted sleep patterns, clashing with internal hormone timing becomes a vicious circle. Poor sleep interferes with the diurnal variation of cortisol, which peaks as an awakening response. Disruption of this cortisol awakening response can disrupt subsequent night sleeping.
A degree of circadian entrainment is possible. In other words, our hormone clocks can adapt to slight changes in sleeping patterns. For example, getting up early for exercise training. It is also possible to reset internal biological clocks, as we do after a long-haul flight. This is because in our brain we have a biological light sensor which has direct communication with the manager of the hormone orchestra, conveniently situated in very close proximity in the brain. The timing of daily hormone release can be reset to correspond with local night and day timing. This contrasts to the situation of doing shift work, where you are continuously in conflict with night/day timing and internal hormone clocks.
Top tips for sleep to optimise hormone health
So, if there is one behaviour that you are going to improve this year, it should be sleep.
Sleep hygiene is the term used to cover strategies to ensure a good night’s sleep. One of the tops tips is to try and go to bed at a regular time, before midnight. A recent study shows that is these hours before midnight that are particularly valuable for hormone health. In fact, it is useful to set an alarm for going to bed.
Another strategy to help sleep is finding a bedtime “wind down” routine that suits you. For example, reading or listening to music. Looking at mobile electronic devices is not one of these. The reason being that the light emitted from these devices prevents the production of the sleep hormone melatonin.
When it comes to hormone health, sleep is indeed the chief nourisher. Sleep and other lifestyle choices to harness hormones for optimal health, through life, are explored in detail in “Hormones, Health and Human Potential: A guide to understanding your hormones to optimise your health and performance”.
Oscar Wilde quipped that “Moderation is a fatal thing. Nothing succeeds like excess.” However, when it comes to enjoying a healthy lifespan, nothing succeeds like moderation.
Harnessing Hormones through Lifestyle Choices for Health
Personalising Health through Lifestyle
Hippocrates advocated that giving each individual just the right amount of exercise and nourishment, not too little and not too much, is the safest way the health. Although Hippocrates is often known as the father of medicine, more accurately he could be described as the father of health. Health being not just the absence of disease, rather the positive combination of physical, mental and social health.
In ancient Greek times it was not known why moderation, of nutrition and exercise surely lead to health. As I describe in “Hormones, Health and Human Potential” it is the interactions of these behaviours with our hormone networks that maintain internal harmony known as homeostasis. Homeostasis is equilibrium of the internal environment to support all physiological processes for health. Hormone networks can adapt and withstand a certain degree of external excess in the form of too much or too little nutrition or exercise. However there comes a critical point, personal for each individual, where continued excess of unbalanced behaviours will tip over into adverse effects on health. Incidentally in this situation it is not hormones that become unbalanced, rather unbalanced behaviours have forced hormone networks into extensive adaptive changes.
Rebalancing Lifestyle Choices
There are certainly ever emerging challenges for attaining just the right amount and timing of each lifestyle choice around nutrition and exercise. Everyone likes a “quick fix”: apart from your hormones and your health. This is why New Year’s resolutions around extreme dieting or exercise at either end of the spectrum don’t lead to long term benefits. Another problem is that it is difficult to override in-build “safety” mechanisms, so it is challenging psychologically to stick to original intentions. Your body and millions of years of evolution knows best. This can leave you deflated and demotivated. You can’t stick to your plan and this plan does not bring the success you expected. What are the ways to set you on the surest path for optimal heath?
Lifestyle choices for 2023
Exercise
There are two very important factors in your choice of exercise. Firstly, that this is something you personally enjoy. Studies show that those who chose exercise that they enjoy are more likely to keep exercising and make healthy food choices. My personal favourite is taking a ballet class with my excellent teacher and friends of many years. Dance also covers the second important point about exercise choice in that it should involve different types of fitness. I see many people just focusing on a cardiovascular type of exercise, neglecting strength, flexibility and neuromuscular skills. However, if ballet is not your thing, then choose your exercise types wisely for enjoyment and to cover all bases of fitness.
Nutrition
Nutrition is very similar to exercise in that food choices should cover all the nutritional requirements for the individual and not neglect the enjoyment element of eating. Trying to adhere rigidly to any type of diet that does not encompass these elements will not end well for health in the long run. I see a lot of exercisers who end up in unintentional or intentional low energy availability with associated adaptative down regulation of hormones, which can be challenging to rectify. At the other end of the spectrum, for those who maybe have favoured energy intake over energy expenditure, the type of weight reduction diets that purport to give rapid weight loss, can often be counterproductive in the long term. If it sounds too good to be true, it probably is.
Sleep
“Sleep is the chief nourisher in life’s great feast”. Although Shakespeare did not realise at the time of writing “Macbeth”, sleep certainly is the chief nourisher when it comes to hormones. Many hormone biological clocks, biochronometers, are set according to our sleep patterns with recent research showing that lack of sleep adversely impacts hormone health for men and women. So aiming for good sleep patterns is something relatively straight forward and actionable to support health.
Stress management
We often have our own personal responses to “stress”. This could be responding through an excess of behaviour at either end of spectrum: eating and/or exercising too little or too much. Especially when combined with disrupted sleep patterns, this creates the perfect storm for challenging hormone health. This vicious circle can become a repeating pattern of response to “stress”. I put “stress” in inverted commas intentionally, because “stress” is our personal interpretation of external stressors. We each have our own interpretation of events and our personal response.
For this reason, “stress” management strategies are a personal choice. Identifying your personal triggers for deviating away from balanced behaviours is an important starting point. Then noting what tends to be your typical response is to these triggers. Can you explore more helpful ways to deal with your personal triggers? Is this listening to music, reading, mediation, meeting with friends or as Hippocrates advised going for a walk? I often see people (including myself) who have tendency to over exercise when confronted with stress provoking situations. So, in this case, going for more walks wouldn’t be the best option. Make sure your strategies are personal to you.
Moderation for Optimal Health 2023
The top tip for optimal health in 2023 and beyond is to aim for moderation and balance across the key lifestyle choices of exercise, nutrition and sleep. Combined with your personal stress management strategies to avoid too much or too little of any of these behaviours, this is the surest way to health as Hippocrates advised. If you do need to modify or fine tune your choices, making small changes that you can sustain over the whole year and beyond will bring success in health.
In my book “Hormones, Health and Human Potential”, I really enjoyed writing the chapter 5XX “Of Mice and men….and Women!” Celebrating Horme the goddess of effort, energy and action. However, there are some instances where even this formidable goddess is challenged and adaptations are required[1].
Challenges to menstrual cycle hormones
Menstrual cycle hormone choreography is as beautiful as it is complex. Generally, this repeating motif follows the score faithfully during a woman’s reproductive years. However, when external stressors become too great, then menstrual hormone fluctuations respond and adapt.
A single stressor, for example financial concerns or a life event can impact hormones and disrupt menstrual cycles on a short time scale of a handful of cycles. However, a combination of stressors can have a synergistic effect on disrupting female hormone networks. Additive stressors over a long-time scale are known as an allostatic load. A high allostatic load causes a more extensive adaptation of female hormones[2]. For example, a high level of stress from intense exercise training together with metabolic stress from insufficient food intake can result in total suppression of menstrual cycle hormone fluctuation and cessation of periods (amenorrhoea) found in relative energy deficiency in sport (RED-S).
Unbalanced behaviours
Although “hormone imbalance” is a popular phrase, this has no medical meaning. This misleading phrase does a massive disservice to Horme and to millions of years of evolution in fine-tuning the most intricate hormone network. It is not the hormone network that has become “unbalanced”, rather it is our unbalanced behaviours and/or management of external stressors that have caused hormones to adapt and change appropriately. On a positive note, understanding hormones empowers us to nurture and harness our hormones through our lifestyle choices.
Spectrum of female hormone adaptation
There is a graded response of female hormones to external stressors, depending on the number and the time scale of these. A cumulative combination of stressors results in a high allostatic load which causes amenorrhoea. Physiological causes of amenorrhoea must be excluded: pregnancy and menopause; as should medical causes such as prolactinoma and polycystic ovary syndrome (PCOS).
The type of amenorrhoea occurring as an adaptive response to a high allostatic load is functional hypothalamic amenorrhoea (FHA). This means that the neuroendocrine gatekeeper in the brain, the hypothalamus, has taken the executive decision to suspend female hormone fluctuations, in order to conserve resources to deal with the stressful situation. From an evolutionary point of view this is not the time for the high demand state of pregnancy. The good news is that being an adaptive functional response, FHA is reversible if the underlying cause is addressed.
Tip of the iceberg
Amenorrhoea is a very obvious clinical sign. Similarly, oligomenorrhoea (less than 9 periods per calendar year). However, these menstrual disruptions are just the tip of the iceberg. Less obvious are the subclinical ovulatory disturbances (rather unflatteringly referred to as SODs). This is where a women may experience a menstrual period, but the full repertoire of female hormone fluctuation has not occurred. Specifically, progesterone has not increased to levels that would be expected in the luteal phase of the cycle (second half of the cycle). If ovulation has occurred, then the remnant of the egg follicle in the ovary forms the corpus luteum which secretes progesterone. Progesterone increases resting metabolic rate and energy demand. So, keeping progesterone low is a good adaptive response to high allostatic load by keeping energy demand low.
If subclinical ovulatory disturbances are an adaptive physiological response, does this matter for a woman’s health? The answer is yes. Oestradiol (the most active form of oestrogen) often takes the limelight when it comes to positive effects on bone, soft tissue, cardiovascular, and neurological health. However, evidence is emerging that progesterone plays an equally important supporting role in these areas of health. For this reason, it is important to identify these elusive disturbances in menstrual hormone choreography.
How to detect subclinical ovulatory disturbances
As I discuss in my book in the chapter “Hormone Supermodels”, applying artificial intelligence (AI) techniques to modelling menstrual cycle hormones can help in identifying subtleties in hormone disruption. This is a fast-moving field and even since publishing on this topic, further advances are being made as more data is emerging and employment of different mathematical techniques, with reduction in the number of samples required. Monitoring temperature change as surrogate for indicating adequate progesterone levels during the luteal phase is a non invasive way of monitoring menstrual cycle hormone function. Personalisation of female hormone health is on the move. Nevertheless, the cornerstone of any medical AI focused on hormones is the medical doctor with expertise in hormones, putting the results in clinical context for the individual. Explaining and advising with practicality and empathy is vital.
This personalised medical approach is crucial when, by definition, subclinical ovulatory disturbances will require guidance on changing behaviours to reverse adaptive hormone changes. When I work with athletes and dancers experiencing hormone disruption due to imbalances in exercise and nutrition, I find it helpful in referring to recovery from a hormone injury as comparable to recovering from a physical injury. Furthermore, there can be a psychological dimension to subclinical ovulatory disturbances. How we interpret external events and think impact our hormones. For example, cognitive dietary restraint (just thinking you should eat less/be thinner) can cause subclinical ovulatory disturbances.
Nurturing Horme
Menstrual cycle hormone choreography is the most intricate and beautiful of all the hormone networks. There is a spectrum of hormone adaptation according to the degree of “stress” put on the system. The visible tip of the iceburg is menstrual disruption such as amenorrhoea and oligomenorrhoea. Less obvious, beneath the surface are subclinical ovulatory disturbances. Subclinical ovulatory disturbances are adaptive hormone responses to unbalanced behaviours and/or interpretation of external events. These subtleties of subclinical ovulatory disturbances can be challenging to identify. However, it is important to do so and provide appropriate medical support to restore these hormones for long term health.
[1] Keay N. Hormones, Health and Human Potential 2022 Sequoia books
[2] Prior J. Adaptive, reversible, hypothalamic reproductive suppression: More than functional hypothalamic amenorrhea Front. Endocrinol 2022 Sec. Reproduction https://doi.org/10.3389/fendo.2022.893889