If you are striving to reach your peak performance, then the PEAQ can help you reach your personal full potential. Click here to get started on the PEAQ
Matching your energy intake to your energy demands helps you reach your personal peak health and exercise performance. On the other hand, failing to meet your energy demands results in low energy availability. This increases your risk of developing relative energy deficiency (REDs) and its adverse health and performance consequences.
People of any age, whatever their level and type of exercise, can be at risk of developing REDs; from elite dancers and athletes to recreational exercisers.
The PEAQ is a mobile Application that will guide you through a series of questions about exercise, physical characteristics, nutrition, hormone function and well-being. It just takes a few minutes.
Your PEAQ report instantly generates a REDs Risk Score and provides valuable insights into your energy status and potential risks, along with guidance. The PEAQ is intended for those 16 years of age and over.
The PEAQ has been developed based on in several published research studies where the questionnaire responses and scores have been correlated with measurements of hormones and bone health in athletes in various sports [1-7] and dancers [8-12]. These questionnaires were cited in the updated International Olympic Committee (IOC) consensus statement on REDs 2013.
Assessment of Relative Energy Deficiency in Sport, Malnutrition Prevalence in Female Endurance Runners by Energy Availability Questionnaire, Bioelectrical Impedance Analysis and Relationship with Ovulation status. Clinical Nutrition Open Science 2025S.
Body composition, malnutrition, and ovulation status as RED-S risk assessors in female endurance athletes, Clinical Nutrition ESPEN 2023, 58 :720-721
Keay N, Craghill E, Francis G Female Football Specific Energy Availability Questionnaire and Menstrual Cycle Hormone Monitoring. Sports Injr Med 2022; 6: 177
Nicolas J, Grafenuer S. Investigating pre-professional dancer health status and preventative health knowledge Front. Nutr. Sec. Sport and Exercise Nutrition. 2023 (10)
Nicola Keay, Martin Lanfear, Gavin Francis. Clinical application of monitoring indicators of female dancer health, including application of artificial intelligence in female hormone networks. Internal Journal of Sports Medicine and Rehabilitation, 2022; 5:24.
Nicola Keay, Martin Lanfear, Gavin Francis. Clinical application of interactive monitoring of indicators of health in professional dancers J Forensic Biomech, 2022, 12 (5) No:1000380
Mountjoy M, Ackerman KE, Bailey DM et al 2023 International Olympic Committee’s (IOC) consensus statement on Relative Energy Deficiency in Sport (REDs) British Journal of Sports Medicine 2023;57:1073-1098
This article explores the current state of play regarding relative energy deficiency in sport (REDs), highlighting the recent updates from the International Olympic Committee (IOC) consensus statement September 2023. Psychological factors and mental health are recognised as having a reciprocal relationship in both the aetiology and outcome of chronic low energy availability leading to REDs. This has important implications in terms of prevention and management of individuals experiencing REDs. Unintentional or intentional unbalanced behaviours around exercise and nutrition leads to a situation of low energy availability. Low energy availability is not synonymous with REDs. Rather cumulative, sustained low energy availability, particularly low carbohydrate availability, leads to the clinical syndrome of REDs comprising a constellation of adverse consequences on all aspects of health and performance. This situation can potentially arise in both biological sexes, all ages and level of exerciser. This is of particular concern for the young aspiring athlete or dancer, where behaviours are being established and in terms of long-term consequences on mental and physical health. The mechanism of sustained low energy availability leading to these negative health outcomes is through the adaptive down regulation of the endocrine networks. Therefore, raising awareness of the risk of REDs and implementing effective prevention and identification strategies is a high priority.
Introduction
Relative energy deficiency in sport (REDs) was first described in the International Olympic Committee (IOC) consensus statement published in the British Journal of Sports and Exercise Medicine (BJSM) 2014(Mountjoy, 2014). Since then, there have been updates published in 2018 (Mountjoy, 2018) and most recently in September 2023 (Mountjoy, 2023).
Seminal studies of female collegiate runners in 1980s found that those athletes with higher weekly training load, but same food intake as those with lower training load, experienced menstrual disruption, including secondary amenorrhoea and poor bone health (Drinkwater, 1984). This led to the description of the female athlete triad, which comprises a clinical spectrum of eating patterns, menstrual function and bone health. This ranges from optimal fuelling, menstrual function and bone health; to eating disorders, amenorrhoea and osteoporosis.
However, with further evidence emerging it became apparent that the impact of under fuelling is not confined to menstrual and bone health. Rather that the consequences of under fuelling are multisystem and can include male athletes. This led to the initial description of REDs in 2014 as a syndrome comprised of the potential adverse effects on many systems in the body with both physical and mental health implications. Crucially, unlike the female athlete trad, REDs also included the potential negative sequalae on athletic performance. Ultimately the goal for all athletes is to perform to their best, so REDs is not something of interest just in academic or clinical circles. REDs is highly relevant to both biological sexes and all levels and ages of exerciser.
What is Energy Availability?
The underlying aetiology of REDs is low energy availability. The life history theory describes how biological processes compete for energy resources (Shirley, 2022). Energy requirement for movement is prioritised from an evolutionary point of view in order to take evasion action from predators. The residual energy from food intake is described as energy availability. This is roughly equivalent to resting metabolic rate for the individual. Simply lying in bed all day, staying alive, is high energy demand for humans as homeotherms. The numerical value of energy availability is expressed in Kcals/Kg of fat free mass. The energy availability requirement for health will vary between individuals depending on sex, age and body composition. Although energy availability is a very useful concept, in practice is it not actually measured outside of the research setting. Rather objective surrogates indicating energy availability can be measured such as triiodothyronine (T3) which is used as a primary indicator of low energy availability as outlined in the update REDs clinical assessment tool described in further detail below (Stellingwerff, 2023 ).
An important highlight from the updated consensus statement on REDs is that it is specifically low carbohydrate availability that is most detrimental, especially for reproductive hormone networks. Comparing isocaloric intake, where there is a low proportion of energy from carbohydrate, this has the most marked negative consequence on both hormone health and performance. The mechanism of sustained low carbohydrate availability appears to involve the hormone leptin, an adipokine, secreted by adipose tissue. Low levels of leptin cause suppression of the reproductive axis via the hypothalamus-pituitary axis (Keay, 2022).
Aetiology of Low Energy Availability
Low energy availability is a situation where, once energy demand from movement has been met, the residual energy available is insufficient to support the functioning of other biological life process.
Low energy availability could arise unintentionally or intentionally (Keay, 2019). Unintentional low energy availability is where an exerciser does not appreciate the energy demands of exercise and other activities with an energy demand. For example, many athletes will not consider the energy required to “commute” to a training session on foot or bike. Unintentional low energy availability could be due to practical issues: for example, a long cycle ride over several hours will require the cyclist to take nutritional sources in the pockets of clothing and/or plan ahead suitable stops where it is possible to obtain nutrition. Similarly, going on a training camp, especially at altitude, will greatly increase energy demand from exercise and needs to factored in. Finances could also be a limiting factor.
On the other hand, intentional low energy availability is where an exerciser intentionally restricts nutrition intake in the belief that this might confer a performance advantage in terms of body weight, composition or shape. This is particularly associated with any exercise against gravity such as running, road cycling, climbing; weight category sports like martial arts and aesthetic forms of sport (diving, gymnastics) and dance.
For individuals with intentional low energy availability, psychology and mental health can have a reciprocal interaction (Pensgaard, 2023). Those exercisers with personality characteristics such as self-motivation, perfectionism can be very laudable traits in terms of dedication to exercise training to achieve success. However, when these characterises impact and support rigid behaviours around training and nutrition, this can become problematic. This is shown in Figure 1 “Psychological factors in REDs”. Those who are able to adapt to external pressures and have a flexible approach to training and nutrition are more likely to experience positive outcomes. Whereas those who have a more rigid approach, which might include disordered eating and or an eating disorder and/or exercise dependence are more likely to experience negative outcomes. This reinforces self-doubt and culminates in a vicious circle of perpetuating rigid behaviours and negative outcomes in terms of both physical and mental health.
Evidence for this interaction between psychological factors and risk of REDs was found in our study of dancers, referenced in the updated IOC consensus statement. A significant relationship was found between psychological factors such as anxiety around body shape/weight and missing training. These psychological factors in turn had significant associations between physical manifestations of low energy availability (low body weight) and physiological outcomes (menstrual irregularity) (Keay, 2020). Similarly, in more of our published research papers referenced in the IOC consensus statement focusing on male athletes, an significant association was found between cognitive nutritional restraint and negative physiological and performance outcomes (Jorov, 2021).
This reciprocal interaction between internal and external factors is a systems biology approach, highlighted in the recent updated IOC consensus statement. From a physiological point of view the brain is a high energy demand organ, requiring a good supply of glucose. So low carbohydrate availability will restrict this cerebral supply, which can impair cognitive function and ultimately good decision making. It is interesting to reflect that the neuroendocrine gatekeeper, the hypothalamus keeps a watching brief on internal and external factors, not distinguishing between the source of stressors when putting in motion an adaptive response (Keay, 2022).
Consequences of Low Energy Availabiity
Low energy availability is not synonymous with REDs. Indeed, short term low energy availability might initially bring some good performances. Low energy availability becomes problematic depending on the time scale, which in turn determines the degree of adaptive response, described in the clinical physiological model of REDs (Burke, 2023). The first system to adapt to low energy availability is bone: bone turnover moves in favour of resorption over formation. This is why bone stress responses, specifically bone stress fractures, can be an early warning sign of REDs and designated a primary indicator in the updated IOC consensus statement. There will follow sequential down regulation of metabolic rate mediated via the thyroid axis, followed by the reproductive axis. In women primary amenorrhoea or sustained functional hypothalamic amenorrhoea (FHA) of 6 months or more duration is a severe primary indicator of REDs. In men, low rage testosterone is a severe primary indicator. Ultimately body composition will be adversely affected, with the only endocrine system to be up regulated being that of the hypothalamic-pituitary-adrenal axis (Keay, 2019).
Health
Cumulative low energy availability causes the syndrome of REDs, which produces progressive adverse effects on all aspects of health: physical, mental and social, described in the REDs conceptual model. Poor sleep will compound these negative health effects (Keay, 2022).
Performance
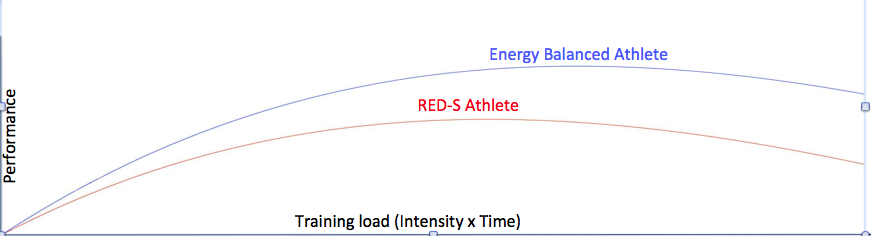
Although there may be some initial good performances, chronic low energy availability will result in adverse performance consequences of REDs, described in the REDs performance conceptual model. In our referenced papers in the consensus statement, we found that in male athletes, short term low energy availability impacted performance (Jurov, 2022). In another of our referenced studies we showed that male cyclists in sustained low energy availability over 6 months, not only experienced bone loss commensurate to astronauts in space, but these cyclists also underperformed compared to their energy replete fellow cyclists (Keay, 2019). On a positive note, explaining to athletes and dancers that improving energy availability will improve their performance, can help in overcoming problematic behaviours.
Identification of those at risk
In view of the potential adverse health and performance effects of REDs, it is a priority to raise awareness of this risk to affect prevention. To this end the British Association of Sports and Exercise Medicine (BASEM) has a website health4performance.co.uk dedicated to providing reliable information on REDs for athletes, parents, coaches and health care professionals together with BASEM endorsed online courses. Targeting and identifying those at increased risk is very important. Young athletes and dancers can be most severely affected as down regulation of hormone function due to low energy availability can cause delay in growth and development. In particular, delayed puberty and menarche dampens the accrual of peak bone mass, with implications for bone health (Keay, 2000). Furthermore, there is evidence that these adverse effects on bone health might not be fully reversible (Keay, 1997)
From a psychological point of view, the young aspiring athlete and dancer is also at heightened risk. Explored and viewed by many dancers in “The Dark Side of Ballet Schools” Panorama (season 33, episode 28). Selection for specialised training will inevitably favour those who are self-motivated and dedicated. In a group of individuals sharing similar psychological traits this could act as a “breeding ground” for reinforcing these characteristics in ways that could lead to behaviours which are not conducive to positive outcomes. Rather reinforcing the negative interpretation of external and internal factors, leading to a vicious circle of reinforcing attitudes and behaviours leading to REDs, as described in Figure 1
Risk stratification
Early identification of those at risk of developing REDs is an important preventative strategy. Especially for young aspiring athletes and dancers where behaviours around eating and exercise are being developed and established. A step-by-step approach is provided in the updated version 2 of the Relative Energy Deficiency in sport Clinical Assessment Tool (REDsCat v2) to identify and risk stratify individuals (Stellingwerff, 2023 ). Initial, low cost, screening questionnaires can be helpful, particularly if tailored to a specific sport/activity or dance. For example: sports specific energy availability questionnaire (SEAQ) (Keay, 2018) and dance energy availability energy questionnaire (DEAQ) (Keay, 2020). This can be helpful in identifying those individuals where further investigation is clinically indicated. As REDs is a diagnosis of exclusion, targeted blood testing excludes medical conditions per se and provide objective quantification in the stratification of risk. Severe primary indicators of REDs are issues in the reproductive axis: long duration of amenorrhoea in females and low range testosterone in males.
From a combination of all these results the individual can be placed in an appropriate risk category. The updated REDs CAT v2 includes a finer grained approach with four categories from green, yellow, amber to red.
This assessment also provides the background on which to base the appropriate level of support. For all, management will be directed at restoring energy availability and include modification of training and nutritional intake. However, the details will vary according to the severity of REDs. Individuals with intentional REDs, especially when formally diagnosed with an eating disorder, will need most intensive input than a person with transient unintentional low energy availability.
Management
A nuanced approach is required for individual athletes, depending on their risk stratification and biopsychosocial factors. In all cases some degree of psychological support will be helpful. Involvement of the extended multidisciplinary team is ideal: medical doctor, dietician, coach and parent (where appropriate) with the athlete/dancer at the centre.
In order to restore energy availability this will require careful discussion around nutrition in terms of consistency of eating patterns and composition of food groups consumed. This starts with regular meals containing good portions of complex carbohydrate and protein. Studies show that inconsistent intake of carbohydrate (eg “backloading” eating to the evening) produces an unfavourable hormone profile. Fuelling around training is also a high priority for hormone health and driving positive adaptations to exercise. Pre training consumption of carbohydrate together with post training refuelling with both complex carbohydrate and protein within 20 minutes of stopping are important behaviours for favourable hormone response to exercise (Keay, 2022).
In terms of pharmacological intervention, NICE guidelines have been updated 2022 in recommending body identical hormone replacement therapy (HRT) over the combined oral contraceptive pill (COCP) for bone protection in those with evidence of bone poor health due to functional hypothalamic amenorrhoea (FHA) as a consequence of REDs (BASEM, 2023). Poor bone health is defined as age matched Z score < -1 of the lumbar spine (trabecular bone particularly sensitive to low oestradiol) and/or 2 or more stress fractures at a site of concern (trabecular rich bone). For male athletes/dancers external testosterone is not appropriate as this supresses internal hormone production. Furthermore, testosterone is on the world anti-doping authority (WADA) banned list and it is not possible to obtain a therapeutic use exemption (TUE) as REDs is a functional condition, not a medical condition.
Prevention
Prevention is always the ultimate goal. In order to achieve this aim, a cultural shift in sport and dance is required. Emphasis on the fact that health is a prerequisite for performance. Pursuing a lighter body weight or leaner body composition will not automatically lead to improved performance. Each individual will have a personal tipping point. As we are all different, there is no such thing as a generic “ideal” weight/shape/body composition.
In practical terms, prevention can be considered as primary, secondary and tertiary (Torstveit, 2023). Primary prevention consists of providing and disseminating reliable educational resources. Secondary prevention includes early identification of those at risk of developing REDs, together with prompt and correct diagnosis. For example, regardless of whether an athlete or dancer, amenorrhoea in a woman of reproductive age (apart from physiological amenorrhoea of pregnancy) is never “normal”; whether blood tests are in range, or not. The tertiary level of prevention encompasses evidence-based treatments. As mentioned above, NICE guidelines are now in line with Endocrine Society and IOC in advising temporising HRT for bone protection in FHA. Not the COCP which masks underlying hormone dysfunction and is not bone protective. Similarly, thyroxine is not advised where there is downregulation of this axis as a consequence of REDs. This is not the same as the medical condition of a primary underactive thyroid indicated by raised thyroid stimulating hormone (TSH) (Keay, 2022).
Conclusion
Ultimately, we all have a role to play in supporting exercisers, athletes and dancers in avoiding “the REDs card” (Mountjoy, 2023). This involves the extended multidisciplinary team, starting with the individual exerciser, family, friends and coaches. Then bringing in health care professionals from medicine, dietetics and physiotherapy.
Imbalances in behaviours around exercise and nutrition can have potential negative consequences on all aspects of health and performance. On a positive note, exercise, supported with appropriate nutrition, is an excellent way to achieve and maintain optimal physical, mental and social health and support performance. This is applicable for all ages and levels of exercisers from the recreational to the amateur and elite athlete.
References
Burke LM, Ackerman KE, Heikura IAet al. Mapping the complexities of Relative Energy Deficiency in Sport (REDs): development of a physiological model by a subgroup of the International Olympic Committee (IOC) Consensus on REDs British Journal of Sports Medicine 2023;57:1098-1108.
Drinkwater B, Nilson K, Chesnut C. Bone Mineral Content of Amenorrheic and Eumenorrheic Athletes N Engl J Med 1984; 311:277-281 DOI: 10.1056/NEJM198408023110501
Jurov I, Keay N, Hadžić V et al. Relationship between energy availability, energy conservation and cognitive restraint with performance measures in male endurance athletes. J Int Soc Sports Nutr 2021;18:24. doi:10.1186/s12970-021-00419-3
Jurov I, Keay N, Spudić D et al. Inducing low energy availability in trained endurance male athletes results in poorer explosive power. Eur J Appl Physiol 2022;122:503–13. doi:10.1007/s00421-021-04857-4
Keay N, Overseas A, Francis G. Indicators and correlates of low energy availability in male and female dancers BMJ Open Sport & Exercise Medicine 2020;6:e000906. doi: 10.1136/bmjsem-2020-000906
Keay N, Francis G. Infographic. Energy availability: concept, control and consequences in relative energy deficiency in sport (RED-S) British Journal of Sports Medicine 2019;53:1310-1311.
Keay N, Rankin A. Infographic. Relative energy deficiency in sport: an infographic guide
British Journal of Sports Medicine 2019;53:1307-1309.
Keay N, Francis G, Hind K. Low energy availability assessed by a sport-specific questionnaire and clinical interview indicative of bone health, endocrine profile and cycling performance in competitive male cyclists BMJ Open Sport & Exercise Medicine 2018;4:e000424. doi: 10.1136/bmjsem-2018-000424
Keay N, Francis G, Entwistleet al. Clinical evaluation of education relating to nutrition and skeletal loading in competitive male road cyclists at risk of relative energy deficiency in sports (RED-S): 6-month randomised controlled trial BMJ Open Sport & Exercise Medicine 2019;5:e000523. doi: 10.1136/bmjsem-2019-000523
Keay N. The modifiable factors affecting bone mineral accumulation in girls: the paradoxical effect of exercise on bone. Nutrition Bulletin 2000, 25: 219-222. https://doi.org/10.1046/j.1467-3010.2000.00051.x
Keay N, Fogelman I, Blake G. Bone mineral density in professional female dancers.
British Journal of Sports Medicine 1997;31:143-147.
Mountjoy M, Ackerman KE, Bailey Det al. 2023 International Olympic Committee’s (IOC) consensus statement on Relative Energy Deficiency in Sport (REDs) British Journal of Sports Medicine 2023;57:1073-1097.
Mountjoy M, Ackerman KE, Bailey Det al. Avoiding the ‘REDs Card’. We all have a role in the mitigation of REDs in athletes British Journal of Sports Medicine 2023;57:1063-1064.
Pensgaard AM, Sundgot-Borgen J, Edwards Cet al. Intersection of mental health issues and Relative Energy Deficiency in Sport (REDs): a narrative review by a subgroup of the IOC consensus on REDs British Journal of Sports Medicine 2023;57:1127-1135.
Stellingwerff T, Mountjoy M, McCluskey Wet al. Review of the scientific rationale, development and validation of the International Olympic Committee Relative Energy Deficiency in Sport Clinical Assessment Tool: V.2 (IOC REDs CAT2)—by a subgroup of the IOC consensus on REDs British Journal of Sports Medicine 2023;57:1109-1118.
International Olympic Committee relative energy deficiency in sport clinical assessment tool 2 (IOC REDs CAT2) British Journal of Sports Medicine 2023;57:1068-1072.
Shirley M, Longman D, Elliott-Sale K et al. A Life History Perspective on Athletes with Low Energy Availability. Sports Med 2022 52, 1223–1234. https://doi.org/10.1007/s40279-022-01643-w
Todd E, Elliot N, Keay N. Relative energy deficiency in sport (RED-S) British Journal of General Practice 2022; 72 (719): 295-297. DOI: https://doi.org/10.3399/bjgp22X719777
Torstveit M, Ackerman K, Constantini N et al. Primary, secondary and tertiary prevention of Relative Energy Deficiency in Sport (REDs): a narrative review by a subgroup of the IOC consensus on REDs Br J Sports Med 2023;57:1119–1126.
Long-term low energy availability leads to adaptive changes throughout the body resulting in the clinical outcomes of REDs
Earlier this week the updated consensus statement from the International Olympic Committee (IOC) on relative energy deficiency in sport (REDs) 2023 was published in the British Journal of Sport Medicine (BJSM)[1]. What are the key points from the range of papers presented in this issue dedicated to REDs?
What’s in a name change?
Making “s” lower case is helpful as relative energy deficiency is not limited to those involved in sport. You can still be at risk of REDs even if you would not consider yourself an athlete; rather “just” someone that does regular exercise. Furthermore, most genres of dance are not sport, yet dancers are another group who can be at risk.
Time scale of low energy availability
The type of adaptive responses to low energy availability is dependent on the temporal component of this energy deficient. Energy availability is the amount of energy “available” once demand from exercise has been accounted for. If this available energy is not sufficient to maintain all the “housekeeping” physiological processes, then the body will respond by going into “eco” mode and down regulating body systems[2]. A small, short-term energy deficit may not be problematic. We have all been in situations where eating patterns don’t go according to plan. For example, a particularly busy time at work, disruption to travel plans, or lack of food availability.
However, sustained, cumulative energy deficit can lead to progressive adaptation shown in the figure.
These adaptive changes across many body systems have adverse outcomes on both health and performance. This is REDs. The clinical syndrome of health and performance consequences of long-term low energy availability. This is what happened in our study of male cyclists referenced in the BJSM publication. We quantified the negative effects of low energy availability on hormone networks, bone health and performance in male cyclists[3]. Those cyclists in low energy availability lost bone mass commensurate with an astronaut in space for 6 months and underperformed in races[4]. This negative impact of low energy availability on performance was underlined in our other studies of male athletes, referenced in the IOC papers [5,6]. Ultimately these are particularly important findings for athletes and their coaches, where performance is the priority.
Menstrual cycles
This concept of a gradated adaptive response to the combined effects of training load, nutrition and recovery can be applied when considering the spectrum of reproductive axis responses in female athletes and dancers, ranging from eumenorrhoea, subclinical ovulatory disturbances to functional hypothalamic amenorrhoea[7] shown in figure of Subclinical Ovulatory Disturbance. Functional hypothalamic amenorrhoea (FHA) is potentially just the tip of the iceberg when it comes to adaptive change to low energy availability. Report of menstruation and even signs of ovulation, may belie suboptimal production of progesterone. As progesterone increases metabolic rate, low production could be considered an early response to low energy availability. This hypothesis is currently being tested in a study of dancers, funded by the British Association of Sport and exercise Medicine.
Carbohydrate availability
Although we talk about low energy availability, the updated IOC consensus statement highlights that carbohydrate availability is the key. This is based on evidence that carbohydrate is the main substrate for exercise above a certain intensity. Furthermore, the hormones of the reproductive axis are particularly sensitive to carbohydrate availability. The IOC statement highlights studies, where despite isocaloric diets, those low in carbohydrate resulted in hormone disruption and poorer athletic performance outlined in the statement.
Health is essential for performance
Another important theme is that optimal health is a prerequisite for performance. This includes both physical and mental aspects of health. Many of the psychological characteristics of athletes and dancers can predispose individuals to developing REDs. For example, although dedication, perfectionism and motivation are laudable qualities, these can spill over into behaviours around training and nutrition. This can be associated with exercise dependence and disordered eating patterns.
If an individual is anxious about body shape, weight and food, this can have a negative health outcome. For example, in our study of dancers[8], quoted as a reference in the updated IOC statement, we found that there were significant relationships between anxiety about controlling weight and eating and missing training, and physical outcomes of low BMI and physiological health in terms of lack of regular menstrual cycles. Regular menstrual cycles in women are a barometer of internal healthy hormones. Similarly in another referenced study, we found that cognitive restraint in male athletes had an adverse effect on hormone profiles[9]. How you think impacts hormone health. This interaction is shown by the reversible arrow between psychological factors as both a driver and result of REDs shown in the updated REDs health conceptual model.
Weighty matter
Weight is a measurement of gravity, not athletic potential. Being a certain weight or body composition does not guarantee athletic success. This fact was emphasised by the lead author of the special edition on REDs on the BJSM podcast. Realistically most types of exercise will involve overcoming gravity, nevertheless, there comes a tipping point where being too light weight and/or having too low body fat means being unhealthy and compromising both physical and mental performance. Furthermore, we are all individuals so our personal optimal weight and body composition will be personal to each of us. Not the generic “lighter is faster”.
Identification
Ultimately low energy availability is a concept and not measured outside of research settings. Rather, making a diagnosis of REDs is a diagnosis of exclusion. In other words, other potential medical conditions must be excluded. This can be achieved through a process of identifying those at risk with energy availability questionnaires, followed by assessing clinical symptoms and signs: such as growth trajectories in young athletes and menstrual status in female athletes and dancers. Readily available and reliable investigations such as blood tests and DXA scans are outlined. These clinical findings have been presented as primary, severe indicators (hypothalamic reproductive disruption in men and women), primary indicators, secondary indicators and other supportive factors.
When considering hormone tests is really important to emphasise that even if a result is not out of range, where the result lies in the range is crucial. Together with considering hormones as networks providing a pattern that is informative. For example, in correctly identifying subclinical down regulation of the thyroid or reproductive axis[2].
Risk stratification
Each of indicators described in the consensus statement carries a score, so that an individual can be risk stratified. The REDsCAT2 has a finer grained zone compromising of green, yellow, orange and red, replacing the 3 zoned traffic light system.
Clinical management
Ultimately as the underlying aetiology of REDs is low energy availability, then the aim of supporting an individual experiencing REDs is to restore sufficient energy availability through a combination of nutrition and possibility reducing demand from intense training. As this will involve behaviour change, this can be challenging and a multidisciplinary team approach is advised. Highlighted for female athletes experiencing functional hypothalamic amenorrhoea (FHA) and associated poor bone health, that the combined oral contraceptive pill is not advised. Rather for bone protection in the short-term HRT (transdermal oestradiol and cyclic micronised progesterone) is recommended in line with updated NICE guidelines in UK[10].
The risk of low energy availability and REDs in dancers will be dicsuused at the forthcoming British Association of Sports and Exercise Medicine annual conference 6/10/23. https://health4performance.basem.co.uk/
3 Keay N, Francis G, Hind K Low energy availability assessed by a sport-specific questionnaire and clinical interview indicative of bone health, endocrine profile and cycling performance in competitive male cyclists. BMJ Open Sport Exerc Med 2018;4:e000424. doi:10.1136/bmjsem-2018-000424
4 Keay N, Francis G, Entwistle I et al Clinical evaluation of education relating to nutrition and skeletal loading in competitive male road cyclists at risk of relative energy deficiency in sports (RED-S): 6-month randomised controlled trial BMJ Open Sport & Exercise Medicine 2019;5:e000523. doi: 10.1136/bmjsem-2019-000523
5 Jurov I, Keay N, Spudić D et al Inducing low energy availability in trained endurance male athletes results in poorer explosive power. Eur J Appl Physiol 2022;122:503–13. doi:10.1007/s00421-021-04857-4
6 Jurov I, Keay N, Rauter S Reducing energy availability in male endurance athletes: a randomized trial with a three-step energy reduction. Journal of the International Society of Sports Nutrition 2022;19:179–95. doi:10.1080/15502783.2022.2065111
7 Keay N. Interactions of the female hormone network, exercise training and nature of adaptation. ResearchGate. June 2023 DOI: 10.13140/RG.2.2.28787.71204
8 Keay N, Overseas A, Francis G Indicators and correlates of low energy availability in male and female dancers. BMJ Open Sport ExercMed 2020;6:e000906. doi:10.1136/bmjsem-2020-000906
9 Jurov I, Keay N, Hadžić V et al Relationship between energy availability, energy conservation and cognitive restraint with performance measures in male endurance athletes. J Int Soc Sports Nutr 2021;18:24. doi:10.1186/s12970-021-00419-3
Although improvements are being made in raising awareness and in effective medical management of relative energy deficiency in sport (RED-S)[1, 2] what about once an athlete/dancer is “medically cleared” to return to sport/dance? What advice/support is there for athletes/dancers and their coaches/teachers? After discussions with coaches, here are some suggestions on how to achieve return to sport/dance after RED-S.
To recap, RED-S is a situation of low energy availability (LEA), which can lead to adverse health and performance consequences[3,4]. LEA can be a result of intentional energy restriction, which covers a spectrum of issues with eating from disordered eating to full blown clinical eating disorder. Ironically the original intention of these eating issues may have been to improve athletic performance, yet sustained LEA will ultimately lead to stagnation and deterioration in performance as found in male athletes[5].
The desire to return to full fitness can be a powerful incentive to address LEA. Nevertheless return to sport/dance needs to be carefully structured in collaboration with coaches to prevent injury and avoiding regression to the LEA state.
Structured return to training and nutrition
Initially focus should be on body weight strength and conditioning (S&C). Inevitably in RED-S adaptive responses to training stimuli will be dampened due to shut down of hormones networks into an energy saving mode. Once adequate EA has been established, hormone networks will be able to respond. Restoring muscle tone and working on proprioception forms a good basis to build from to mitigate injury risk. Impaired neuromuscular skills have been reported in female athletes in LEA[6], together with adverse effects of LEA on bone health increases injury risk.
The other reason for gradual return to training is that a routine of fuelling around training (before, during, after) needs to be established. In particular recovery nutrition within 30 minutes window to enable hormonal responses to training. Note that having this recovery nutrition does not mean reducing intake at the next meal!
Long endurance should be eased into after restoring muscle strength and control, in order to prevent injury. Additionally this type of training will necessitate a higher energy requirement. If adequate energy availability has only recently been restored, the balance is fragile and so too much training too soon can have negative effects. Especially if a fuelling strategy around training has not been established as described above.
High intensity/interval training should be the last type of training to be resumed as this places the highest stress and requires the highest energy demand on the athlete/dancer.
Injury, soft tissue and bone stress responses are more frequent in hormonal dysfunction of RED-S in both male and female athletes[7]. If an injury has been sustained during this period of LEA then particular emphasis needs to be on initial S&C. In the case of previous bone stress responses, multi-direction loading is key to build bone strength before resuming formal run training in athletes who are runners. Even if a bone injury has not occurred, bone turnover is one of the first systems to be adversely impacted by RED-S, so including this type of multidirectional bone loading in the initial structured return for all athletes/dancers would be beneficial.
Discuss with your coach a realistic, attainable goal if this will help. Maybe a low key race/event several months down the track
What to look out for
Don’t ignore injury niggles, illness or fatigue. Discuss with your coach and back off if necessary. This is a process, not a sprint.
Female athletes. You may well have experienced menstrual disruption during your time in LEA. This is a crucial training metric. Please use it! If your menstruation becomes irregular/stops this is your warning sign that your body is not ready to step up training[7]. Male coaches please reinforce this and be aware of this point. Remember Gwen Jorgensen posting her periods on Training Peaks as a training metric?
Flexibility in approach. Try not to put pressure on yourself to return to your previous PBs. It is important to have a plan, but you can be flexible. Everyone is different so this process of returning to sport/dance does not have a set, rigid timetable.
Enjoyment! Don’t forget the original reason that you started your sport/dance was for enjoyment! This is an opportunity to rediscover that joy, whether you return to competition or not.
“Recovery?” Does anyone fully “recover” from disordered eating/eating disorder? I don’t think so. To be a successful athlete, or indeed successful in life you need self-motivation, drive, determination. All admirable qualities, but sometimes these can get diverted to cause unhealthy eating/training patterns. So be aware that in times of stress it may be tempting to revert to old habits of under eating/over exercise to reassure yourself that you are in control.
Be prepared for questions: why have you been off training? Why are you not doing fully training schedule? Maybe you want to tell your team mates/friends. Maybe you don’t. That is your call.
So good luck with your return to sport/dance after RED-S, if that is what you want to do. Always discuss with you coach how to approach this.
5 Reduced Neuromuscular Performance in Amenorrheic Elite Endurance Athletes.
Tornberg Å Melin A Koivula F Johansson A Skouby S et. al.Medicine and science in sports and exercise 2017 vol: 49 (12) pp: 2478-2485
6 Low Energy Availability Is Difficult to Assess but Outcomes Have Large Impact on Bone Injury Rates in Elite Distance Athletes Heikura, Ida A. Uusitalo, Arja L.T. Stellingwerff, Trent et al International Journal of Sport Nutrition and Exercise Metabolism 2018, 28, 4, 403-411
Menstrual periods are a barometer of healthy hormones. The evolutionary purpose of ovulation is to reproduce. Furthermore the carefully biologically choreographed variation of hormones that occurs during an ovulatory menstrual cycle is crucial to health and athletic performance.
Why? Hormones are chemical messengers that have far reaching effects throughout the body and drive the beneficial adaptations to exercise. In the case of menstrual cycles, the fluctuations of oestrogen and progesterone are key to this process. The effects of these sex steroids go far beyond reproduction. These hormones play important roles in bone strength, cardiovascular health, optimal lipid profile and production of neurotransmitters to regulate mood. The effects of low levels of oestrogen and progesterone are well documented in menopausal women who experience loss in bone mass, risk of osteoporosis and fracture, together with an increase risk of cardiovascular disease.
Some definitions
Amenorrhoea=lack of menstrual cycles
Menarche= start of menstrual cycles
According to the Royal College of Obstetrics and Gynaecology
Primary Amenorrhoea: no onset of menstrual cycles by age 16 years.
Secondary amenorrhoea: cessation of menstrual cycles in a previously regularly menstruating woman for > 6months
Oligomenorrhoea: < 9 menstrual cycles per calendar year
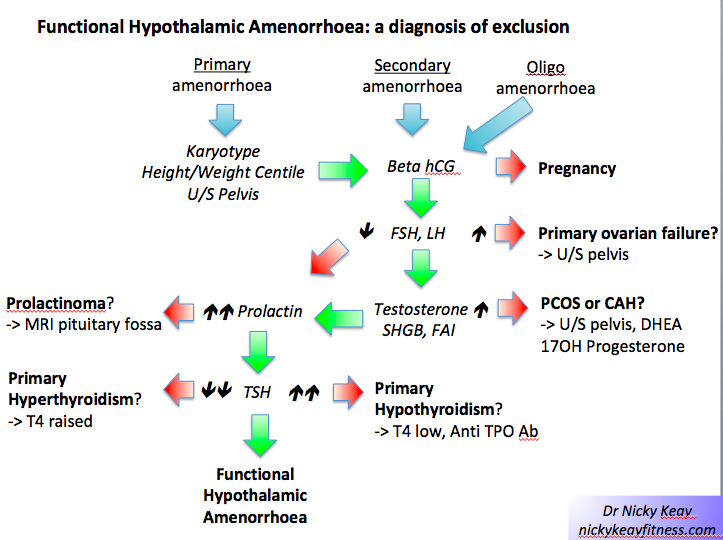
Any form of amenorrhoea requires medical investigation to exclude an underlying medical condition. The most common medical causes of amenorrhoea are polycystic ovary syndrome (PCOS), prolactinoma, thyroid conditions and other endocrine conditions. Functional hypothalamic amenorrhoea (FHA) is a diagnosis of exclusion. In other words before arriving at a diagnosis of FHA [1], medical conditions that could potentially cause amenorrhoea have to be ruled out.
Relative energy deficiency in sport (RED-S) is a situation of low energy availability (LEA) that can be unintentional or intentional as a result of a mismatch between energy intake and energy requirement. The two sources of energy demand arise from exercise training load and maintenance of fundamental physiological function across multiple body systems [2]. In female athletes/dancers with RED-S the most obvious clinical sign is amenorrhoea as a result of FHA. In all cases of RED-S the management strategy is directed to address the underlying issue of LEA [3].
In female athletes/dancer with FHA due to RED-S, there is the possibility of pharmacological intervention based on the RED-S Clinical Assessment Tool [4]. In other words evidence from DXA of Z-score of lumbar spine < -1 and/or stress fracture. What are the most effect hormonal interventions in such cases?
What’s in a name? It is every woman’s right to choose the form of contraception she wishes to use. Hormonal contraception provides a convenient method. The combined oral contraceptive pill (OCP) contains oestrogen and progesterone to prevent ovulation. The OCP produces regular withdrawal bleeds in response to these external hormones. Progesterone-only contraception can be taken orally, via implant or delivered by an intrauterine coil and typically does not produce withdrawal bleeds. As with any medication there are potential side effects, which have to be weighed up against the benefits. Regarding the effect of hormonal contraception on bone in young menstruating women, there is evidence that such medication can impair bone health [5].
The OCP produces regular withdrawal bleeds. These are NOT menstrual periods; ovulation is prevented. Rather the OCP causes withdrawal bleeds driven by external non-physiological hormones, as opposed to internally physiologically produced hormones. This is a reason why the OCP is not recommended in FHA, as this medication will mask what is happening with internal hormones [6]. In other words the barometer of healthy hormones has been removed when taking the OCP.
Furthermore, studies show that the OCP can impact other hormone systems that play a role in bone health. The OCP is taken orally thereby producing first pass effects in the liver. These effects include induction of liver enzymes and increased production of binding proteins for hormones. Binding proteins reduce the freely available active form of hormones such insulin like growth factor 1 (IGF-1). This effect is particularly marked in those OCP with non-physiological ethinyl oestradiol. In the case of RED-S there is already a low level of active IFG-1, due to the general suppression of the hypothalamic-pituitary axis.
Therefore in addition to masking FHA, the OCP can also further decrease IGF-1 and thus compound the negative effect on bone. This has been shown to be the case in the clinical setting where the OCP was found to have no bone protective effect on bone mineral density (BMD) in women with FHA. Rather hormone replacement therapy (HRT) consisting of transdermal physiological oestrogen with cyclic micro-ionised progesterone was found to have a positive effect on BMD [7 , 8]
Therefore, if hormonal treatment is to be used in RED-S, HRT (transdermal oestradiol and cyclic micro-ionised progesterone) is best clinical practice. This decision requires careful discussion with the athlete/dancer clarifying that HRT should only be a short-term measure to protect bone health whilst the underlying issue of LEA is being resolved. Behavioural measures relating to training load, nutrition and recovery are essential to restore global hormonal function.
OCP V HRT
• What? Both provide oestrogen and progesterone, but in different forms: non-physiological v physiological
• Why? Purpose of the OCP is to suppress production of endogenous female hormones and prevent ovulation. Purpose of HRT is to replace the physiological amount and form of oestrogen and progesterone
• How? The OCP decreases levels of active, unbound IGF-1. Not bone protective in FHA of RED-S. HRT shown to improve BMD in FHA of RED-S
What to do? Hormonal contraception is a choice for women. In some medical conditions where there is adequate/excess oestrogen such as endometriosis or PCOS, hormonal contraception is effective in clinical management. However in the case of FHA, in particular when occurring as a consequence of LEA in RED-S there is evidence that the OCP is not bone protective and masks the clinical sign of menstruation.
The priority in managing RED-S is to address LEA. If bone protection is required, whilst addressing LEA, HRT (transdermal oestrogen and cyclic progesterone) is best clinical practice.
References
[1] Joy, E., De Souza, M. J., Nattiv, A., Misra, M., Williams, N. I., Mallinson, R. J., … Borgen, J. S. (2014). 2014 Female Athlete Triad Coalition Consensus Statement on Treatment and Return to Play of the Female Athlete Triad. Current Sports Medicine Reports, 13(4), 219–232. https://doi.org/10.1249/JSR.0000000000000077
[2] Mountjoy, M., Sundgot-Borgen, J., Burke, L., Carter, S., Constantini, N., Lebrun, C., … Ljungqvist, A. (2014). The IOC consensus statement: Beyond the Female Athlete Triad-Relative Energy Deficiency in Sport (RED-S). British Journal of Sports Medicine, 48(7), 491–497. https://doi.org/10.1136/bjsports-2014-093502
[3] Mountjoy, M., Sundgot-Borgen, J. K., Burke, L. M., Ackerman, K. E., Blauwet, C., Constantini, N., … Budgett, R. (2018). IOC consensus statement on relative energy deficiency in sport (RED-S): 2018 update. British Journal of Sports Medicine, 52(11), 687–697. https://doi.org/10.1136/bjsports-2018-099193
[4] Mountjoy, M., Sundgot-Borgen, J., Burke, L., Carter, S., Constantini, N., Lebrun, C., … Ackerman, K. (2015, April 1). Relative energy deficiency in sport (RED-S) clinical assessment tool (CAT). British Journal of Sports Medicine. BMJ Publishing Group. https://doi.org/10.1136/bjsports-2015-094873
[5] Beksinska M, Smit J, Hormonal contraception and bone mineral density. Expert Review of Obstetrics & Gynecology, 2011 vol: 6 (3) pp: 305-319
[6] Gordon, C. M., Ackerman, K. E., Berga, S. L., Kaplan, J. R., Mastorakos, G., Misra, M., … Warren, M. P. (2017). Functional hypothalamic amenorrhea: An endocrine society clinical practice guideline. Journal of Clinical Endocrinology and Metabolism, 102(5), 1413–1439. https://doi.org/10.1210/jc.2017-00131
[7] Ackerman, K. E., Singhal, V., Baskaran, C., Slattery, M., Campoverde Reyes, K. J., Toth, A., … Misra, M. (2018). Oestrogen replacement improves bone mineral density in oligo-amenorrhoeic athletes: A randomised clinical trial. British Journal of Sports Medicine. BMJ Publishing Group. https://doi.org/10.1136/bjsports-2018-099723
[8] Singhal, V., Ackerman, K. E., Bose, A., Torre Flores, L. P., Lee, H., & Misra, M. (2018). Impact of Route of Estrogen Administration on Bone Turnover Markers in Oligoamenorrheic Athletes and its Mediators. The Journal of Clinical Endocrinology & Metabolism. https://doi.org/10.1210/jc.2018-02143
Traditionally dance medicine has been somewhat the poor relation of sports medicine. Why is this the case? There is no doubt that dancers, of whatever genre, require the physical and psychological attributes of athletes. However, dance involves an additional artistic component where ultimately performance on stage is judged not according to a score card as in aesthetic sports, rather on the ability of the dancers to forge an emotional connection with the audience.
As with athletes, injuries are always an important topic for dancers: how to recognise the aetiology of injuries and thus develop prevention strategies. Dance UK have published two reports on national enquiries into the health of dancers. Dance UK has now evolved into the organisation One Dance which includes the National Institute of Dance Medicine and Science (NIDMS). One Dance provides delivery of the Healthier Dancer Programme (HDP) whose talks regularly engage 1500+ dancers and dance professionals per year and which will be a part of the One Dance UK conference at the end of November, an overarching event for the entire dance sector. One Dance holds a list of healthcare professionals with experience and expertise in dance. One Dance is an especially an important resource for independent dancers who will not have access to the provision for those working in larger dance companies.
However, beyond injury management, there are important aspects of the health of dancers which need to be considered, highlighted in an information booklet “Your body, Your risk” from Dance UK. The female athlete triad is well established as a clinical spectrum comprising of disordered eating, menstrual dysfunction and impaired bone health. Indeed impaired bone mineral density many persist even after retirement in female dancers. The recent evolution of the female athlete triad into relative energy deficiency in sports (RED-S) provides an important clinical model. RED-S includes male athletes/dancers, involves multiple body systems and crucially, evidence of detrimental effects on athletic performance is being researched and described. In other words RED-S is not restricted to female dancers/athletes with bone stress injuries.
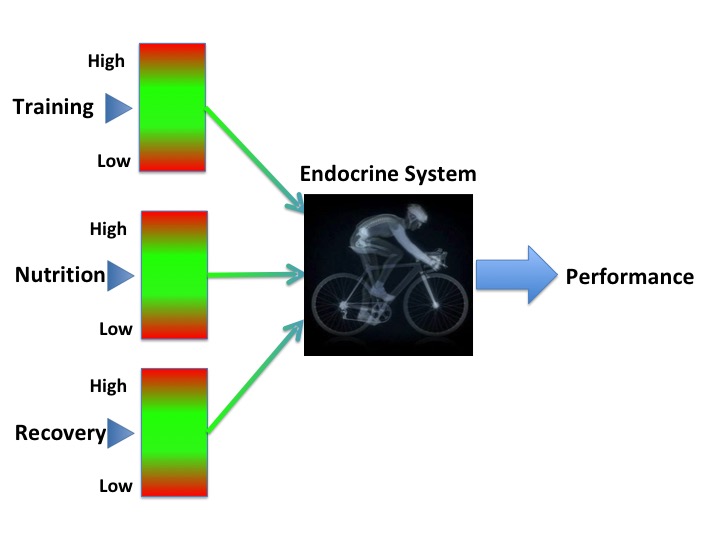
Integrated periodisation of training, nutrition and recovery support perforamnce
The fundamental cause of RED-S is low energy availability where nutritional intake is insufficient to cover energy requirements for training and resting metabolic rate. In this situation the body goes into energy saving mode, which includes shut down of many hypothalamic-pituitary axes and hence endocrine network dysfunction. As hormones are crucial to backing up adaptations to exercise training, dysfunction will therefore have an effect not just on health, but on athletic performance. In dance, neuromuscular skills and proprioception are key for performance. Hence, of concern is that these skills are adversely impacted in functional hypothalamic amenorrhoea, which together with impaired bone health from RED-S, greatly increases injury risk.
Low energy availability can arise in dance and sport where low body weight confers an aesthetic and/or performance advantage. There is no doubt that being light body weight facilitates pointe work in female dancers and ease of elevation in male dancers. Thus, low energy availability can occur intentionally in an effort to achieve and maintain low body weight. Low energy availability can also be unintentional as a result of increased expenditure from training, rehearsal and performance demands and the practicality of fuelling. This situation is of particular concern for young dancers in training, as this represents a high energy demand state, not just for full time training, additionally in terms of energy demands for growth and development, including attainment of peak bone mass.
Despite the significance of RED-S in terms of negative consequences on health and performance, as outlined by the IOC in the recent consensus update, further work is required in terms of raising awareness, identification and prevention. Fortunately these issues are being addressed with the development of an online educational resource on RED-S for athletes/dancers, their coaches/teachers/parents and healthcare professionals which is backed by British Association of Sport and Exercise Medicine (BASEM) and with input from One Dance and NIDMS. In terms of research to facilitate the proliferation of evidence base in dance medicine, One Dance lists calls for research, whilst NHS NIDMS clinics provide access to clinical dance medicine. The importance of the application of this growing field of dance medicine and science for the health and performance of dancers was recently outlined in an article “Raising the barre: how science is saving ballet dancers“.
On the international stage, the International Association for Dance Medicine & Science (IADMS) strives to promote an international network of communication between dance and medicine. To this end, IADMS will hold its 28th Annual Conference in Helsinki, Finland from October 25-28, 2018. In addition to extensive discussion of dance injuries, there will be presentations on “Sleep and Performance” and “Dance Endocrinology”.
So maybe Dance Medicine and Science is not so much the poor relation of Sports Medicine, rather showing the way in terms of integrating input between dancers, teachers and healthcare professionals to optimise the health of dancers and so enable dancers to perform their full potential.
What updates are presented in the IOC consensus statement on RED-S 2018?
Prevention
Awareness is the key to prevention. Yet RED-S continues to go unrecognised. Less than 50% of clinicians, physiotherapists and coaches are reported as able to identify the components of the female athlete triad. In a survey of female exercisers in Australia, half were unaware that menstrual dysfunction impacts bone health. Note that these concerning statistics relate to the female athlete triad. Lack of awareness of RED-S in male athletes is even more marked. RED-S as a condition impacting males, as well as females, was described in the initial IOC consensus statement published in 2014. However there is evidence of the occurrence of RED-S in male athletes pre-dating this.
Identification
Identifying an athlete/dancer with RED-S is not always straight forward. In dance or sports where being light weight confers a performance or aesthetic advantage, how can a coach/teacher distinguish between athletes who have this type of physique “naturally” and those who have disordered eating and are at risk of RED-S? Equally, low energy availability could be a result either of intentional nutrition restriction to control body weight and composition, or an unintentional consequence of not matching an increase in energy expenditure (due to increased training load), with a corresponding increase in energy intake.
Performance effects
Performance is paramount to any athlete or dancer. Apart from physical ability, being driven and determined are important characteristics to achieve success. If weight loss is perceived as achieving a performance advantage, then this can become a competitive goal in its own right: in terms of the individual and amongst teammates. This underlies the interactive effect of psychological factors in the development and progression in the severity of RED-S.
There is both theoretical and practical evidence that short term low energy availability impairs athletic performance as the body is less able to undertake high quality sessions and benefit from the physiological adaptations to exercise. Within day energy deficits have been shown to have adverse effects in both male and female athletes in terms of impact on oestradiol/testosterone and cortisol concentrations. Failure to refuel with carbohydrate and protein promptly after a training session in male runners has been shown to have an adverse effect on bone turnover markers.
To underline the adverse performance effect of low energy availability, a recent study demonstrated that in female athletes, those with functional hypothalamic amenorrhea displayed decreased neuromuscular performance compared to their eumenorrhoeic counterparts. This adverse effect on performance is of particular concern where such skills are crucial in precisely those sports/dance where RED-S is most prevalent. Clearly this situation puts such athletes at increased injury risk, especially if associated with adverse bone mineral density (BMD) due to low energy availability.
Ironically the long term consequences of low energy availability produce adverse effects on body composition: increased fat/lean and reduction in BMD. In other words, the precise opposite effects of what an energy restricted athlete is trying to achieve. In terms of bone health, the lumbar spine is most sensitive to nutrition/endocrine factors (apart from rowers where mechanical loading can attenuate BMD loss at this site in RED-S). Suboptimal BMD is associated with an increased risk of bone injury and therefore impaired performance.
Keay BJSM 2017
Medical Assessment
Low energy availability is the fundamental issue driving the multi-system dysfunction in the endocrine, metabolic, haematological, cardiovascular, gastrointestinal, immunological and psychological systems in RED-S. However, there are practical issues with directly quantifying energy availability as this is subject to the inaccuracies of reliably measuring energy intake and output. Endocrine and metabolic markers have been shown to more objective indicators of low energy availability, which in turn are correlated to performance outcomes such as bone stress injury in male and female athletes. In the case of female athletes there is an obvious clinical indicator of sufficient energy availability: menstrual cycles. As there is no such obvious clinical sign in male athletes is this why RED-S is less frequently recognised? In both female and male athletes there is some degree of clinical variation: there is no absolute threshold cut off with a set temporal component of low energy availability resulting in amenorrhoea or low testosterone in males. Therefore the IOC recommends that individual clinical evaluation include discussion of nutrition attitudes and practices, combined with menstrual history for females and endocrine markers for male and female athletes will give a very clear indication if an athlete is at risk of/has RED-S.
Management
RED-S is a diagnosis of exclusion. Once medical conditions per se have been excluded, RED-S presents a multi-system dysfunction caused by a disrupted periodisation of nutrition/training/recovery. For an athlete the motivation to address these imbalances is to be in a position reach their full athletic potential. This attainment is compromised in RED-S.
Pharmacological interventions are not recommended as first line management in amenorrhoeic athletes. Oral contraception (OCP) masks amenorrhoea with withdrawal bleeds. OCP does not support bone health and indeed may exacerbate bone loss by suppressing further IGF-1. Although transdermal oestrogen, combined with cyclic progesterone does not down regulate IGF-1, nevertheless any hormonal intervention cannot be a long term solution, as bone loss will continue if energy availability is not addressed as a priority.
What next?
The IOC statement suggests further research should include studies with allocation of athletes to intervention groups, with assessment of effects over a substantial time period. Currently a study of competitive male road cyclists over a training/competition season is being undertaken to evaluate the effects of nutrition advice and off bike skeletal loading exercise. Crucially outcome measures will not only be based on bone health and endocrine markers, but measures of performance in terms of power production and race results.
To raise awareness and build support pathways as recommended in the IOC statement, this is an on going process which requires communication between athlete/dancers, coaches/teachers, parents and healthcare professionals both medical and non medical working with male and female athletes.
The action of the sun on skin is the most effective way of making vitamin D. However, even walking around outside naked for 5 hours every day during UK winter months is not sufficient to make adequate vitamin D. Therefore, much to the relief of the audience at the recent BASEM Spring conference, this was not a strategy recommended by Dr Roger Wolman.
Vitamin D is a fat soluble steroid hormone. The majority of which is synthesised in the skin when exposed to ultraviolet B in sunlight, with a small contribution from dietary sources: this vitamin D3 molecule is then hydroxylated twice in the liver and then kidney to produce the metabolically active form of vitamin D. This activated steroid hormone binds to vitamin D receptors in various tissues to exert its influence on gene expression in these cells. The mono hydroxylated form of vitamin D is measured in the serum, as this has a long half life.
Does it matter having low levels of circulating vitamin D during winter months? What are the solutions if moving to warmer climates during the winter is (unfortunately) not feasible? What are the other hormones interact with vitamin D?
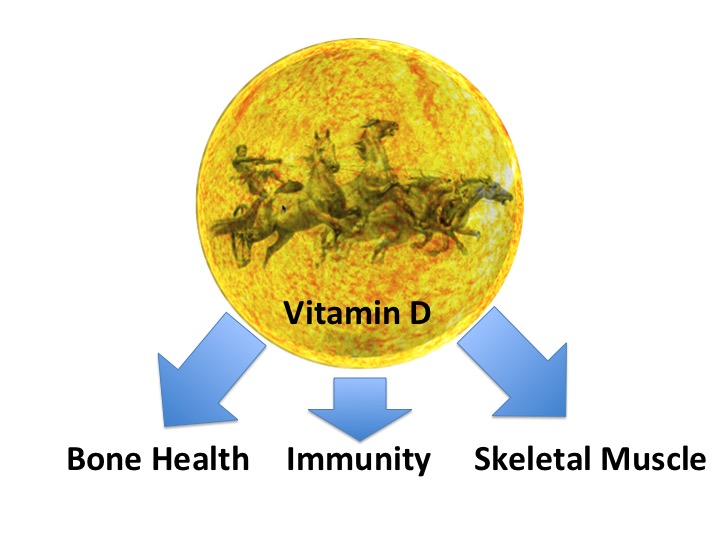
What are the beneficial effects of vitamin D, particularly in the athletic population?
Bone
Rickets and osteomalacia are conditions where vitamin D deficiency results in bone deformities and radiographic appearances are characterised by Looser zones, which in some ways are similar in appearance to stress fractures.
In a large prospective study of physically active adolescent girls, stress fracture incidence was found to have an inverse relationship with serum vitamin D concentrations. In adult female Navy recruits monitored during an 8 week training programme, those on vitamin D supplementation had a 20% reduction in stress fracture. However, oestrogen status was a more powerful risk factor at 91% in those recruits reporting amenorrhoea. Vitamin D is, itself, is a steroid hormone with range of systemic effects. As will be discussed below, its interaction with the sex steroid oestrogen has an important effect on bone turnover.
Immunity
Although sanatoriums, for those suffering with tuberculosis, were based on providing patients with fresh air, any beneficial effect was probably more due to vitamin D levels being boosted by exposure to sunlight. Certainly there are studies demonstrating the inhibitory effect of vitamin D on on slow growing mycobacteria, responsible for TB. What about the influence of vitamin D on other types of infection? In a recent publication, evidence was presented that supplementation with vitamin D prevented acute respiratory tract infections. This effect was marked in those with pre-existing low levels of vitamin D. In a study of athletes a concentration of 95 nmol/L was noted at the cut off point associated with more or less than one episode of illness. In another randomised controlled study of athletes, those supplemented with 5,000IU per day of vitamin D3 during winter displayed higher levels of serum vitamin D and had increased secretion of salivary IgA, which could improve immunity to respiratory infections.
Muscle
There is evidence that supplementing vitamin D3 at 4,000IU per day has a positive effect on skeletal muscle recovery in terms of repair and remodelling following a bout of eccentric exercise. In the longer term, dancers supplemented with 2,000IU over 4 months reported not only reduction in soft tissue injury, but an increase in quadriceps isometric strength of 18% and an increase of 7% in vertical jump height.
Synergistic actions of steroid hormones
No hormone can be considered in isolation. This is true for the network interaction effects between the steroid hormones vitamin D and oestrogen. In a study of professional dancers, there was found to be significant differences in serum vitamin D concentrations in dancers from winter to summer and associated reciprocal relationship with parathyroid hormone (PTH). In situations of vitamin D deficiency this can invoke secondary hypoparathyroidism. Although low levels of vitamin D were observed in the dancers, this was not a level to produce this condition. However, there was an increase in soft tissue injury during the winter months that could, in part, be linked to low vitamin D levels impacting muscle strength.
The novel finding of this study was that female dancers on the combined oral contraceptive pill (OCP) showed significant differences, relative to their eumenorrhoeic counterparts not on the OCP, in terms of higher levels of vitamin D and associated reductions of bone resorption markers and PTH. The potential mechanism could be the induction by the OCP of liver enzymes to increase binding proteins that alter the proportion of bound/bioactive vitamin D.
This interaction between steroid hormones oestrogen and vitamin D could be particularly significant in those in low oestrogen states such as postmenpoausal women and premenarchal girls. Menarche can be delayed in athletes, so is there a case for vitamin D supplementation in young non-menstruating athletes? What is the situation for men? Do testosterone and vitamin D have similar interactions and therefore implications for male athletes with RED-S, where testosterone can be low?
Vitamin D is not simply a vitamin. It is a steroid hormone with multi-system effects and interactions with other steroid hormones, such as sex steroids, which are of particular relevance to athletes.
Endocrine and Metabolic aspects of Sports and Exercise Medicine are crucial determinants of health and human performance, from reluctant exerciser through to elite athlete and professional dancer. This is what the recent BASEM spring conference set out to demonstrate. The previous blog described functional disruption of Endocrine networks caused by non-integrated periodisation of the three key lifestyle factors of exercise/training, nutrition and recovery/sleep, can lead to adverse effects on health and athletic performance.
Integrated periodisation of exercise, nutrition, recovery for optimisation of health and performance (Keay BJSM 2017)
Grace, aesthetic line and ethereal quality belie the athletic prowess required in ballet. What are the Endocrine, metabolic and bone health consequences for this unique group of athletes? Dr Roger Wolman (Medical Advisor to National Institute for Dance Medicine and Science) returned to the important topic of insufficient energy availability in sport/dance where being lightweight confers a performance advantage, resulting in dysfunction in multiple endocrine axes. Dr Wolman discussed his recent research studies in dancers revealing an intriguing synergistic action between oestrogen and vitamin D, which is itself a steroid hormone. Evidence was presented to demonstrate how being replete in vitamin D has beneficial effects on bone, immunity and muscle function. Thus it is key in preventing injury and supporting health in athletes, with particular relevance in premenarchal and postmenopausal women, who are in relative oestrogen deficient states. This presentation will certainly change my clinical practice and, I am sure, that of many in the audience, in ensuring that athletes/patients are vitamin D replete. This may have to be achieved in the form of strategic use of sports informed vitamin D supplementation, given that even walking naked for 5 hours a day outside during UK winter, would not stimulate enough vitamin D production. Therefore, to the relief of many in the audience, Dr Wolman did not recommend this strategy.
Dr Kate Ackerman (member of RED-S IOC working group) explained why we should all tap into our inner endocrinologist. Sport and Exercise Medicine (SEM) goes far beyond diagnosing and treating injury. Is there any underlying endocrine cause for suboptimal health, performance or injury? Be this an endocrine diagnosis that should not be missed, or a functional endocrine dysfunction due to relative energy deficiency in sports (RED-S). Dr Ackerman explained the importance of the multidisciplinary team in both identifying and supporting an athlete experiencing the consequences of RED-S. New research from Dr Ackerman’s group was presented indicating the effects of RED-S on both health and athletic performance.
Females now have combative roles alongside their male counterparts. What are the implications of this type of intensive exercise training? Dr Julie Greaves (Research Director of the ministerial women in ground close combat research programme) presented insightful research revealing that differences in the geometry of bone in men and women can predispose towards bone stress injury and account for increased incidence in this type of injury in female recruits.
Lunchtime discussion and debate was focused on the determinants of athletic gender, lead by Dr Joanna Harper and Professor Yannis Pitsiladis (International Federation of Sports Medicine). Rather than relying on genetic sex, testosterone concentration was proposed as the criteria for determining whether an athlete competes in male or female events. That testosterone concentration is linked to performance was demonstrated in a study published last year in the BMJ where female athletes in the upper tertile of testosterone were shown to have a performance advantage in certain strength based track and field disciplines. This could potentially be an objective, functional metric used to determine sporting categories for transgender and intersex athletes. The only current uncertainty is how previously high levels of testosterone seen in male, or intersex athletes would have already had an impact on physiology, if this athlete then wished to compete as female and therefore lower testosterone levels with medication.
Nutrition is a key component in optimising health and performance through the Endocrine system. Dr Sophie Killer (English Institute of Sport) explained practical implications for athletes. In a study stimulating a training camp, there were distinct differences between athletes on different regimes of carbohydrate intake in terms of endocrine markers and psychological effects. Those athletes on restricted carbohydrate intake fared worse.
Insulin insensitivity is the underlying pathological process in developing type 2 diabetes mellitus (T2DM) and metabolic syndrome. What is the crucial lifestyle intervention to combat this? Dr Richard Bracken (Swansea University) presented the science behind why and how exercise improves blood glucose control and therefore ultimately risk of developing the macro and microvascular complications of diabetes. T2DM is an increasing health issue in the population, which has to be addressed beyond reaching for the prescription pad for medication. Dr Bracken outlined some effective strategies to encourage the reluctant exerciser to become more active. Having worked myself in NHS diabetic clinics over many years, this was a key presentation at the conference to demonstrate that SEM goes far beyond a relatively small group of elite athletes. Highlighting the crucial role of physical activity in supporting health and performance through optimisation of endocrine networks: uniting the elite athlete and the reluctant exerciser.
One Road to Rome (BJSM Keay 2017)
Motivate2Move initiative aims to shift the emphasis from treating disease, to preventing disease. Dr Brian Johnson presented the excellent resource for healthcare professionals to encourage, motivate and educate patients in order to consider exercise as an effective and enjoyable way to improve health.
Hormones play a key role in health and human performance, applicable to all levels of exerciser from reluctant exerciser to elite athlete.
Is your training in tune with your hormones and nutrition to optimise your athletic performance?
Hormones are internal chemical messengers regulating all aspects of your health and athletic performance. Discussed at recent BASEM conference “Health Hormones and Human Performance”
Bone health can be at risk if hormone status not optimal
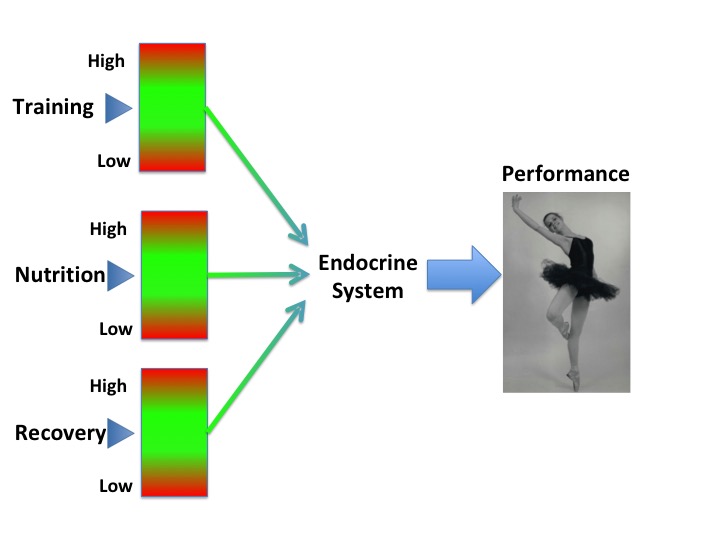
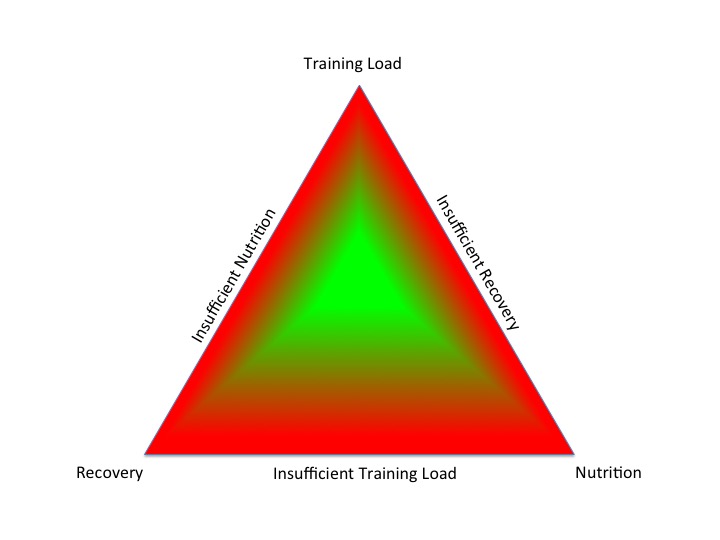
How? To enable your hormones to do the best job they can for your health and sport performance, you need to find a balance between what, how much and when you train, eat and sleep. In the diagram below, this represents staying on the healthy green plateau. Too much, or too little of any of these choices can lead to imbalances and tipping off the green plateau into the red, less healthy peripheries.
Integrated periodisation of training, nutrition and recovery for optimal health and performance (Keay, BJSM 2017)
What? Imbalances between training load, nutrition and recovery can cause problems in the Endocrine system: the whole network of hormone interactions throughout your body. The bottom line is that if insufficient energy is provided through nutrition to cover both your training demands and the “housekeeping” activities within the body to keep you alive, then your body goes into energy saving mode. This situation is called relative energy deficiency in sports (RED-S) and has the potential to adversely impact one or more of the important systems in your body vital for optimal health and performance.
RED-S has evolved from the female athlete triad described in 1980s by Barbara Drinkwater in NEJM, where although female runners were consuming same dietary intake, those with higher training load were more likely to have menstrual dysfunction and low bone mineral density. Since this original description it has become obvious that the reproductive axis is just one of several hormone networks to be impacted by low energy availability and that RED-S also impacts the other half of the population: men.
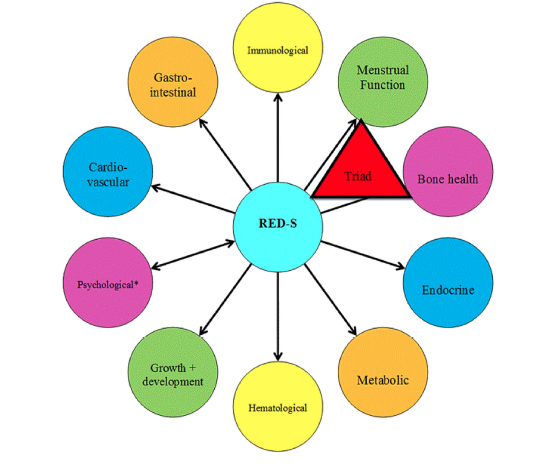
Potential Multisystem effects of RED-S (IOC statement BJSM 2014)
Why? Suboptimal levels of energy availability to support health and performance can arise unintentionally, for example with increased training loads and/or times of growth and development in young athletes. Intentionally restrictive eating patterns can also be the cause of RED-S, particularly in sports/dance where low body weight confers a performance or aesthetic advantage. It is an indisputable fact that in order cycle up a mountain you need to overcome gravity and produce high watts/kg. Equally it is pretty impossible to do pointe work, let alone 32 fouttées en tournant en pointe unless you are a lightweight dancer. However if this at the expense of disrupting your hormones, then the advantage of being low body weight will be lost.
How to know? How to know if you, a teammate or a fellow athlete is at risk of RED-S? If you are a female athlete then your hormones are in balance if you are having regular periods (this does not include withdrawal bleeds as result of being on the oral contraceptive pill). Any woman of reproductive age from 16 years to the menopause should have regular periods (unless pregnant). Regular menstruation acts as the barometer of healthy hormones in women. If this is not the case, whether you are an athlete or not, you need to get this checked out medically to exclude underlying medical conditions. Having excluded these, then you need to review the integrated periodisation of training, nutrition and recovery. In male athletes there is not such an obvious sign that your hormones are at healthy levels. However recurrent injury/illness/fatigue can be warning signs. The diagram below shows all the potential adverse effects of RED-S on performance. Be aware that you do not have to have all, or indeed be aware of any of these effects if you develop RED-S.
Potential Performance effects of RED-S (IOC statement BJSM 2014)
So What? If you are an athlete/dancer, you may be thinking that none of this applies to you. You are feeling and performing fine. Maybe you have not yet experienced any of the detrimental effects of RED-S. However, you will never know how good an athlete you could be and whether you truly are performing to your full potential unless you put yourself in the best position in terms of your hormones to achieve this goal.
Suboptimal performance as result of RED-S (Keay, BJSM 2017)
Key Points
• Insufficient nutrition intake (quantity and quality), whether intentional or not, results in RED-S and multiple hormonal disruptions
• RED-S has detrimental health and athletic performance consequences in both the short and the long term
• Some consequences of RED-S are irreversible for example poor bone health, unless intervention is swift
Check points
• Are you suffering with frequent injuries/fatigue/illness over last 3 months or more?
• Female athletes: if 16 years or older have your periods not started? Have you missed more than 3 consecutive periods?
If yes to any of above, seek medical advice from someone with experience Sports Endocrinology. Now! The longer you leave the situation the harder it will be to rectify. Initially underlying Endocrine conditions per se have to be ruled out. RED-S is a functional dysfunction of the Endocrine system, so a diagnosis of exclusion. Having established RED-S as the diagnosis, monitoring Endocrine markers can be very helpful as these are examples of objective metrics in monitoring energy availability and therefore response to optimising integrated periodisation of nutrition, training and recovery.
Integrated periodisation of key training factors support healthy hormones to drive improvements in performance
What to do? Don’t ignore! Although you may think you are fine, if your hormones are not working for you, then you will never reach your full potential as an athlete/dancer. For female athletes having regular periods means your hormones are in healthy ranges and this is normal. Not starting and/or missing periods is not healthy, for any woman.
For both male and female athletes, if you are experiencing recurrent injury, fatigue or illness, you need to get this checked out. There may be a simple explanation such as viral infection, low vitamin D or iron. However it may be that the underlying reason is due to hormone issues.
If you are an athlete, coach, teacher or parent and concerned that you/an athlete in your care has not got the balance right to optimise health and athletic performance, then a 3 way discussion will help and support the decision to seek medical advice as appropriate.
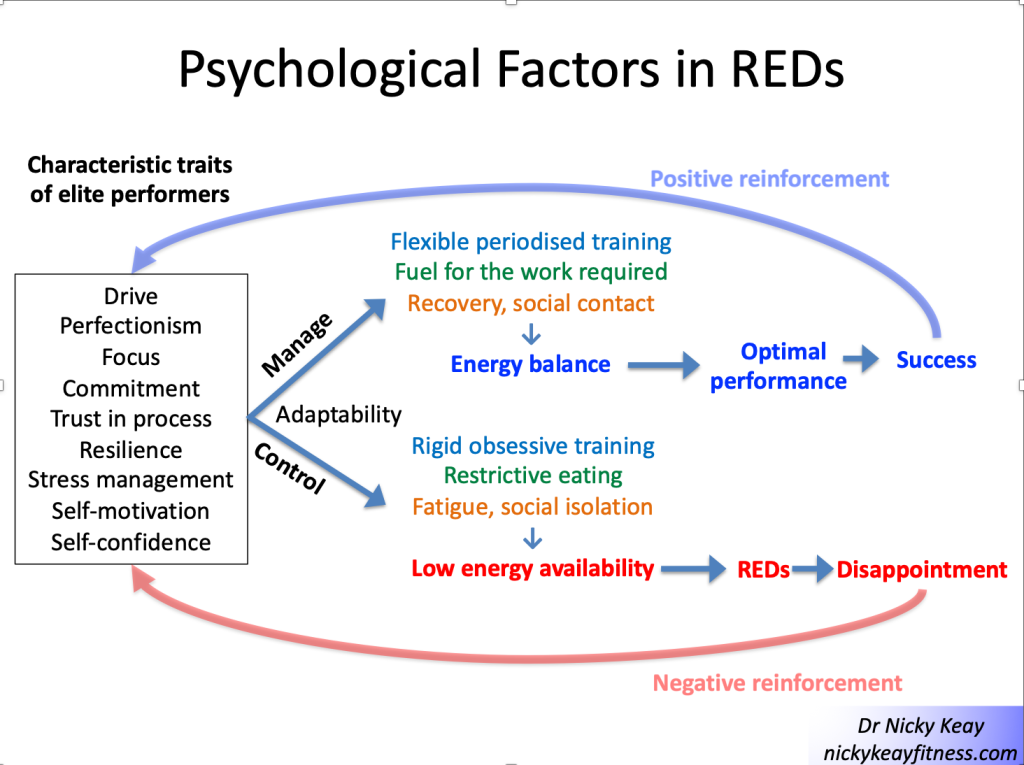
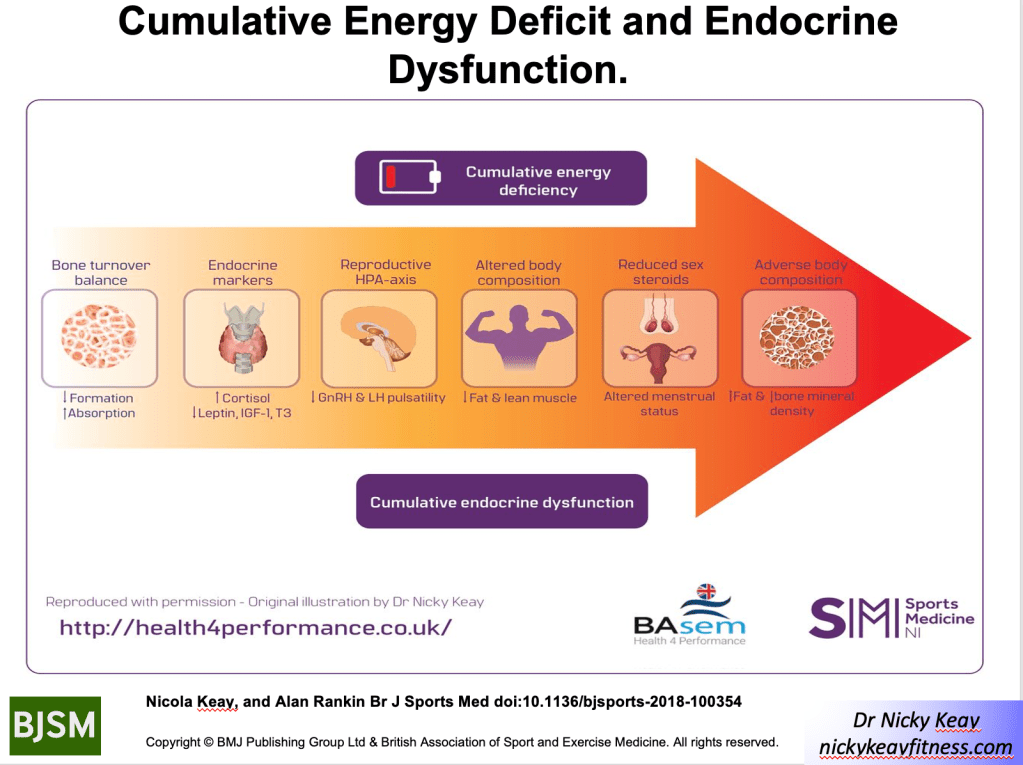
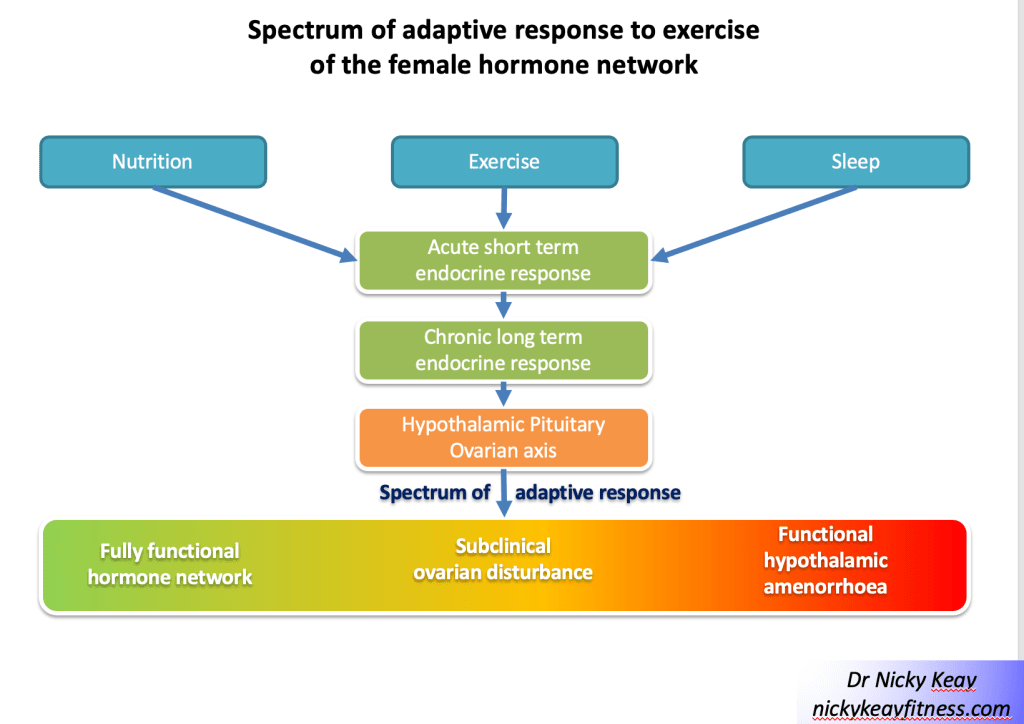
 To recap, RED-S is a situation of low energy availability (LEA), which can lead to adverse health and performance consequences[3,4]. LEA can be a result of intentional energy restriction, which covers a spectrum of issues with eating from disordered eating to full blown clinical eating disorder. Ironically the original intention of these eating issues may have been to improve athletic performance, yet
To recap, RED-S is a situation of low energy availability (LEA), which can lead to adverse health and performance consequences[3,4]. LEA can be a result of intentional energy restriction, which covers a spectrum of issues with eating from disordered eating to full blown clinical eating disorder. Ironically the original intention of these eating issues may have been to improve athletic performance, yet