Returning to Sport/Dance restoring Energy Availability in RED-S?
Although improvements are being made in raising awareness and in effective medical management of relative energy deficiency in sport (RED-S)[1, 2] what about once an athlete/dancer is “medically cleared” to return to sport/dance? What advice/support is there for athletes/dancers and their coaches/teachers? After discussions with coaches, here are some suggestions on how to achieve return to sport/dance after RED-S.
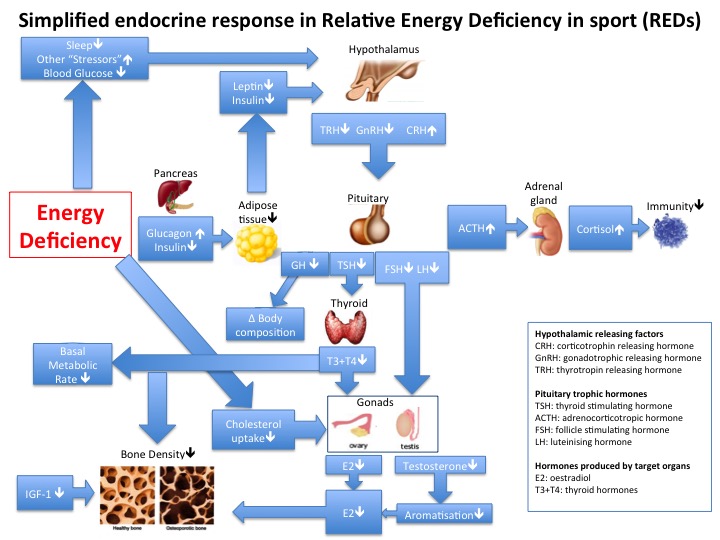
 To recap, RED-S is a situation of low energy availability (LEA), which can lead to adverse health and performance consequences[3,4]. LEA can be a result of intentional energy restriction, which covers a spectrum of issues with eating from disordered eating to full blown clinical eating disorder. Ironically the original intention of these eating issues may have been to improve athletic performance, yet sustained LEA will ultimately lead to stagnation and deterioration in performance as found in male athletes[5].
To recap, RED-S is a situation of low energy availability (LEA), which can lead to adverse health and performance consequences[3,4]. LEA can be a result of intentional energy restriction, which covers a spectrum of issues with eating from disordered eating to full blown clinical eating disorder. Ironically the original intention of these eating issues may have been to improve athletic performance, yet sustained LEA will ultimately lead to stagnation and deterioration in performance as found in male athletes[5].
The desire to return to full fitness can be a powerful incentive to address LEA. Nevertheless return to sport/dance needs to be carefully structured in collaboration with coaches to prevent injury and avoiding regression to the LEA state.
Structured return to training and nutrition
- Initially focus should be on body weight strength and conditioning (S&C). Inevitably in RED-S adaptive responses to training stimuli will be dampened due to shut down of hormones networks into an energy saving mode. Once adequate EA has been established, hormone networks will be able to respond. Restoring muscle tone and working on proprioception forms a good basis to build from to mitigate injury risk. Impaired neuromuscular skills have been reported in female athletes in LEA[6], together with adverse effects of LEA on bone health increases injury risk.
- The other reason for gradual return to training is that a routine of fuelling around training (before, during, after) needs to be established. In particular recovery nutrition within 30 minutes window to enable hormonal responses to training. Note that having this recovery nutrition does not mean reducing intake at the next meal!
- Long endurance should be eased into after restoring muscle strength and control, in order to prevent injury. Additionally this type of training will necessitate a higher energy requirement. If adequate energy availability has only recently been restored, the balance is fragile and so too much training too soon can have negative effects. Especially if a fuelling strategy around training has not been established as described above.
- High intensity/interval training should be the last type of training to be resumed as this places the highest stress and requires the highest energy demand on the athlete/dancer.
- Injury, soft tissue and bone stress responses are more frequent in hormonal dysfunction of RED-S in both male and female athletes[7]. If an injury has been sustained during this period of LEA then particular emphasis needs to be on initial S&C. In the case of previous bone stress responses, multi-direction loading is key to build bone strength before resuming formal run training in athletes who are runners. Even if a bone injury has not occurred, bone turnover is one of the first systems to be adversely impacted by RED-S, so including this type of multidirectional bone loading in the initial structured return for all athletes/dancers would be beneficial.
- Discuss with your coach a realistic, attainable goal if this will help. Maybe a low key race/event several months down the track
What to look out for
- Don’t ignore injury niggles, illness or fatigue. Discuss with your coach and back off if necessary. This is a process, not a sprint.
- Female athletes. You may well have experienced menstrual disruption during your time in LEA. This is a crucial training metric. Please use it! If your menstruation becomes irregular/stops this is your warning sign that your body is not ready to step up training[7]. Male coaches please reinforce this and be aware of this point. Remember Gwen Jorgensen posting her periods on Training Peaks as a training metric?
- Flexibility in approach. Try not to put pressure on yourself to return to your previous PBs. It is important to have a plan, but you can be flexible. Everyone is different so this process of returning to sport/dance does not have a set, rigid timetable.
- Enjoyment! Don’t forget the original reason that you started your sport/dance was for enjoyment! This is an opportunity to rediscover that joy, whether you return to competition or not.
- “Recovery?” Does anyone fully “recover” from disordered eating/eating disorder? I don’t think so. To be a successful athlete, or indeed successful in life you need self-motivation, drive, determination. All admirable qualities, but sometimes these can get diverted to cause unhealthy eating/training patterns. So be aware that in times of stress it may be tempting to revert to old habits of under eating/over exercise to reassure yourself that you are in control.
- Be prepared for questions: why have you been off training? Why are you not doing fully training schedule? Maybe you want to tell your team mates/friends. Maybe you don’t. That is your call.
So good luck with your return to sport/dance after RED-S, if that is what you want to do. Always discuss with you coach how to approach this.
References
1 BASEM Educational website www.health4perforamnce.co.uk
2 BJSM blog: Update on RED-S N Keay 2018
3, 4 IOC consensus statements on RED-S BJSM 2014 and update 2018
5 Reduced Neuromuscular Performance in Amenorrheic Elite Endurance Athletes.
Tornberg Å Melin A Koivula F Johansson A Skouby S et. al.Medicine and science in sports and exercise 2017 vol: 49 (12) pp: 2478-2485
6 Low Energy Availability Is Difficult to Assess but Outcomes Have Large Impact on Bone Injury Rates in Elite Distance Athletes Heikura, Ida A. Uusitalo, Arja L.T. Stellingwerff, Trent et al International Journal of Sport Nutrition and Exercise Metabolism 2018, 28, 4, 403-411
7 What’s so good about Menstrual Cycles? N Keay BJSM blog 2019