One road to Rome: Metabolic Syndrome, Athletes, Exercise
Metabolic syndrome comprises a cluster of symptoms including: hypertension, dyslipidaemia, fatty liver disease and type 2 diabetes mellitus (T2DM).
The underlying pathological process is insulin resistance which distorts metabolism. Temporal and mechanistic connections have been described between hyperinsulinaemia, obesity and insulin resistance. Insulin levels rise, potentially stimulated by excess intake of refined carbohydrates and in addition the metabolic actions of insulin are attenuated on target tissues such as the liver, skeletal muscle and adipose tissue. At a cellular level, inflammatory changes play a part in this metabolic dis-regulation. Mitochondrial action in skeletal muscle is impaired, compromising the ability to oxidise fat as a substrate, thus resulting in muscle glycolysis and a consequent rise in blood lactate.
Although much attention has been focused on restricting calories and treating elevated lipids with medication (statins), evidence is now emerging that this does not have the anticipated effect of reducing mortality from cardiovascular disease. In addition, it has been proposed that the gut microbiota plays a pivotal role in metabolism, inflammation and immunity.
Metabolic syndrome usually conjures an image of an overweight person with or on the verge of developing T2DM. However there is an interesting group of slim people who are also are at risk of developing metabolic syndrome due to insulin resistance. The majority of women with polycystic ovary syndrome (PCOS) present with menstrual disturbance of some description. However not all display the textbook characteristics of Stein-Leventhal syndrome (overweight, hirsute and with skin problems). There is in fact of spectrum of clinical phenotypes ranging from the overweight to the slim. In all phenotypes of PCOS, the crucial uniting underlying metabolic disturbance is insulin resistance. The degree of insulin resistance has been shown to be related to adverse body composition with increased ratio of whole body fat to lean mass.
Although this confuses the picture somewhat, it also simplifies the approach. In all cases the single most important lifestyle modification is exercise.
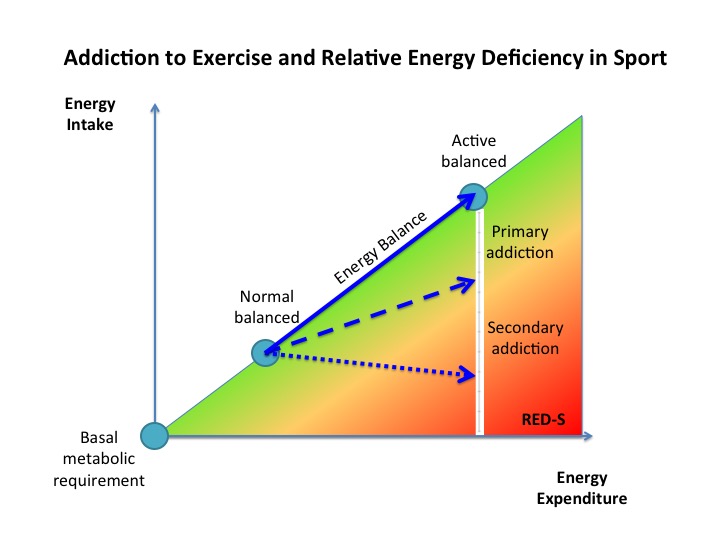
Exercise improves metabolic flexibility: the ability to adapt substrate oxidation to substrate availability. Endurance exercise training amongst athletes results in improved fat oxidation and right shift of the lactate tolerance curve. Conversely metabolic inflexibility associated with inactivity is implicated in the development of insulin resistance and metabolic syndrome.
What about nutritional strategies that might improve metabolic flexibility? Ketogenic diets can either be endogenous (carbohydrate restricted intake) or exogenous (ingestion of ketone esters and carbohydrate). Low carbohydrate/high fat diets (terms often used interchangeably with all types of ketogenic diets) have been shown to improve fat oxidation and potentially mitigate cognitive decline in older people.
However, in the case of athletes, the benefits do not necessarily translate to better performance. Despite reports of such diets enhancing fat oxidation and favourable changes in body composition, a recent study demonstrates that this, in isolation, does not translate into improved sport performance. A possible explanation is the oxygen demand of increased oxidation of fat needs to be supported by a higher oxygen supply. The intermediate group of endurance athletes in this study, on the periodised carbohydrate intake, fared better in performance terms. Another recent study confirmed that a ketogenic diet failed to improve the performance of endurance athletes, in spite of improving fat metabolism and body composition. Despite small numbers, this warrants particular mention as the majority of participants were women, who are in general very underrepresented in scientific studies.
In all likelihood, the reason that these type of diets (ketogenic, high fat/low carb: not always well defined!) did not improve sport performance is that only one aspect of metabolism was impacted and quantified. Although fat oxidation, modified via dietary interventions, is certainly an important component of metabolism, the impact on the interactive network effects of the Endocrine system should be evaluated in the broader context of circadian rhythm. For athletes this goes further, to include integrated periodisation of nutrition, training and recovery to optimise performance, throughout the year.
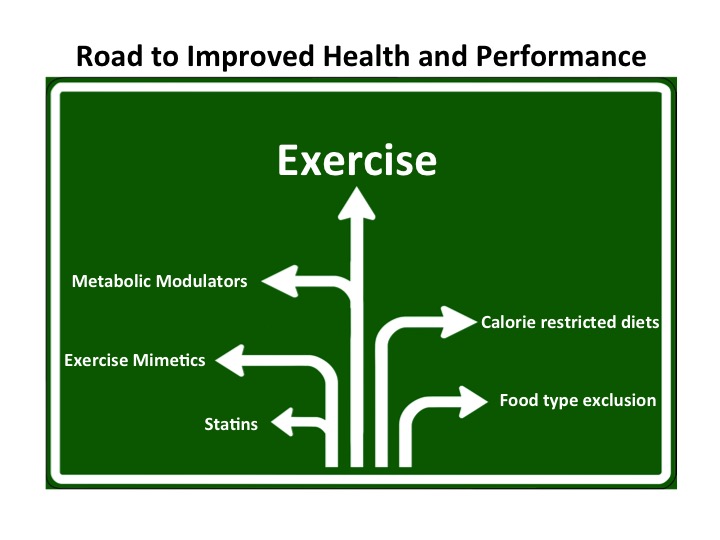
In addition to dietary interventions, medical researchers continue to explore the use of exercise mimetics and metabolic modulators, to address metabolic syndrome. Unfortunately, some have sought their use as a short cut to improved sport performance. Many of these substances appear on the WADA banned list for athletes. However the bottom line is that it is impossible to mimic, either through a dietary or pharmacological intervention, the multi-system, integrated interplay between exercise, metabolism and the Endocrine system.
Only one road to Rome!
Whatever your current level of activity, whether reluctant exerciser or athlete, the path is the same to improve health and performance. This route is exercise, supported with periodised nutrition and recovery. Exercise will automatically set in motion the interactive responses and adaptations of your metabolic and Endocrine systems.
For further discussion on Endocrine and Metabolic aspects of SEM come to the BASEM annual conference 22/3/18: Health, Hormones and Human Performance
References
Insulin action and resistance in obesity and type 2 diabetes Nature Medicine 2017
Inflammation: Why and How Much? Dr N. Keay, British Association of Sport and Exercise Medicine
The cholesterol and calorie hypotheses are both dead — it is time to focus on the real culprit: insulin resistance Clinical Pharmacist 2017
Skeletal muscle mitochondria as a target to prevent or treat type 2 diabetes mellitus Nature Reviews Endocrinology 2016
The essential role of exercise in the management of type 2 diabetes Cleveland Clinic Journal of Medicine 2017
β cell function and insulin resistance in lean cases with polycystic ovary syndrome Gynecol Endocrinol. 2017
The many faces of polycystic ovary syndrome in Endocrinology. Conference Royal Society of Medicine 2017
Association of fat to lean mass ratio with metabolic dysfunction in women with polycystic ovary syndrome Hum Reprod 2014
Sedentary behaviour is a key determinant of metabolic inflexibility Journal of physiology 2017
International society of sports nutrition position stand: diets and body composition J Int Soc Sports Nutr. 2017
A cross-sectional comparison of brain glucose and ketone metabolism in cognitively healthy older adults, mild cognitive impairment and early Alzheimer’s disease Exp Gerontol. 2017
Low carbohydrate, high fat diet impairs exercise economy and negates the performance benefit from intensified training in elite race walkers J Physiol. 2017
Ketogenic diet benefits body composition and well-being but not performance in a pilot case study of New Zealand endurance athletes J Int Soc Sports Nutr. 2017
Sports Endocrinology – what does it have to do with performance? Dr N. Keay, British Journal of Sports Medicine 2017
Hormones and Sports Performance
Endocrine system: balance and interplay in response to exercise training