The state of play on relative energy deficiency in sport (REDs)
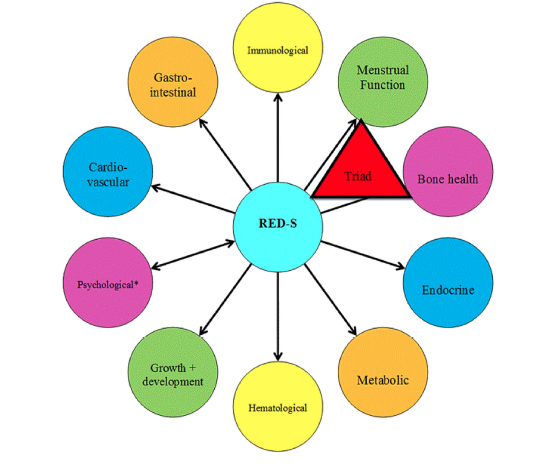
Long-term low energy availability leads to adaptive changes throughout the body resulting in the clinical outcomes of REDs
Earlier this week the updated consensus statement from the International Olympic Committee (IOC) on relative energy deficiency in sport (REDs) 2023 was published in the British Journal of Sport Medicine (BJSM)[1]. What are the key points from the range of papers presented in this issue dedicated to REDs?
What’s in a name change?
Making “s” lower case is helpful as relative energy deficiency is not limited to those involved in sport. You can still be at risk of REDs even if you would not consider yourself an athlete; rather “just” someone that does regular exercise. Furthermore, most genres of dance are not sport, yet dancers are another group who can be at risk.
Time scale of low energy availability
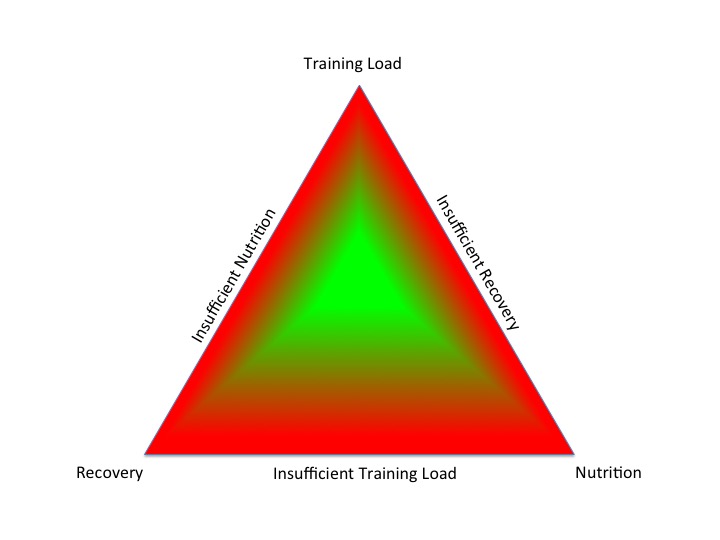
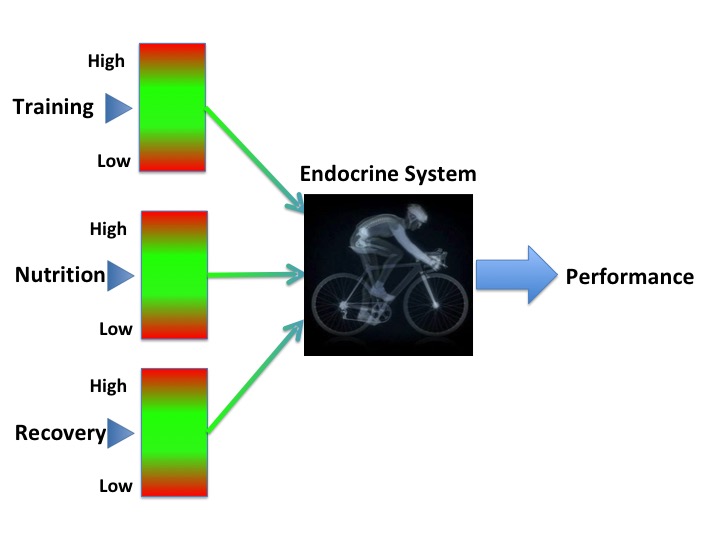
The type of adaptive responses to low energy availability is dependent on the temporal component of this energy deficient. Energy availability is the amount of energy “available” once demand from exercise has been accounted for. If this available energy is not sufficient to maintain all the “housekeeping” physiological processes, then the body will respond by going into “eco” mode and down regulating body systems[2]. A small, short-term energy deficit may not be problematic. We have all been in situations where eating patterns don’t go according to plan. For example, a particularly busy time at work, disruption to travel plans, or lack of food availability.
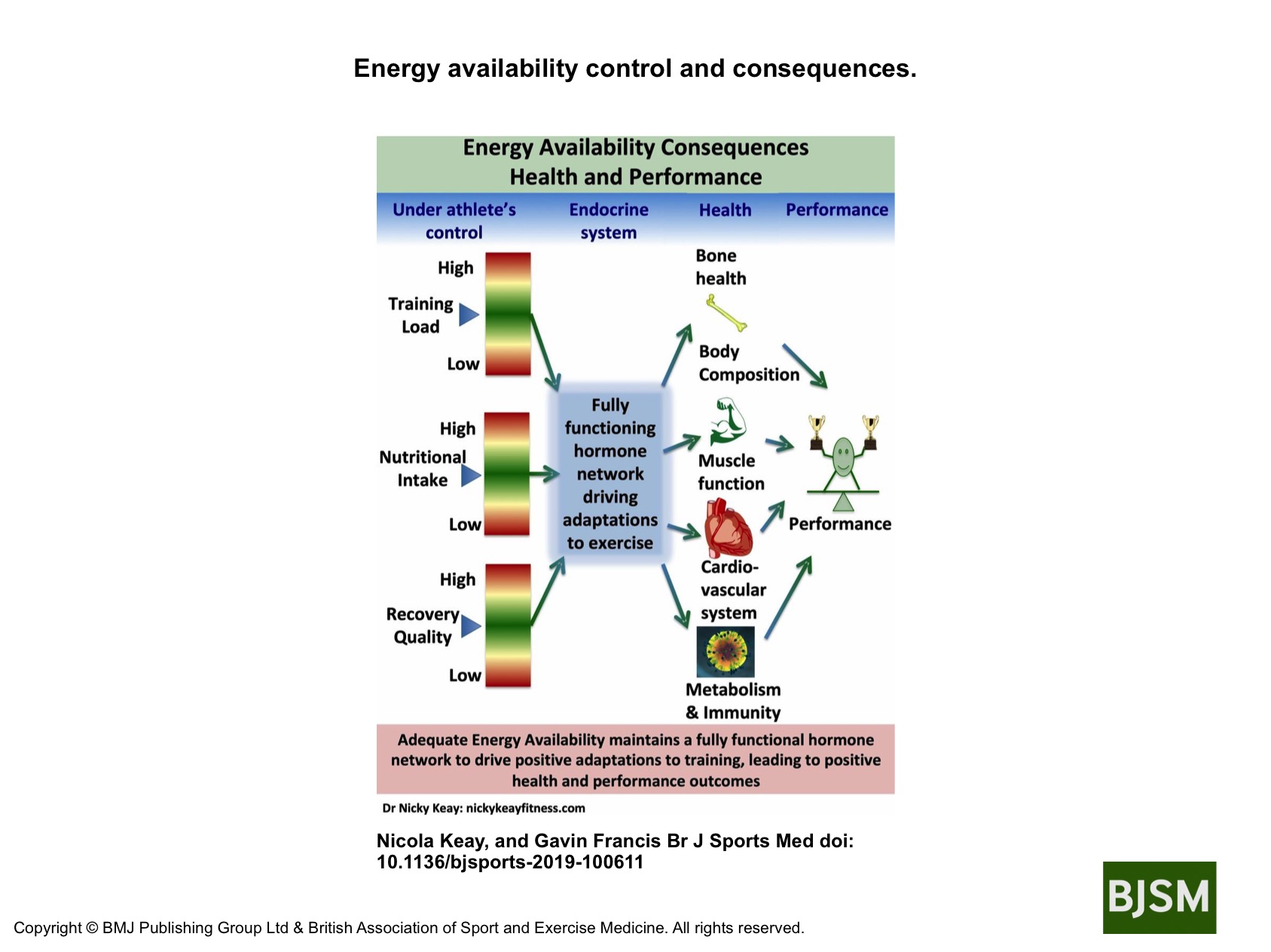
However, sustained, cumulative energy deficit can lead to progressive adaptation shown in the figure.
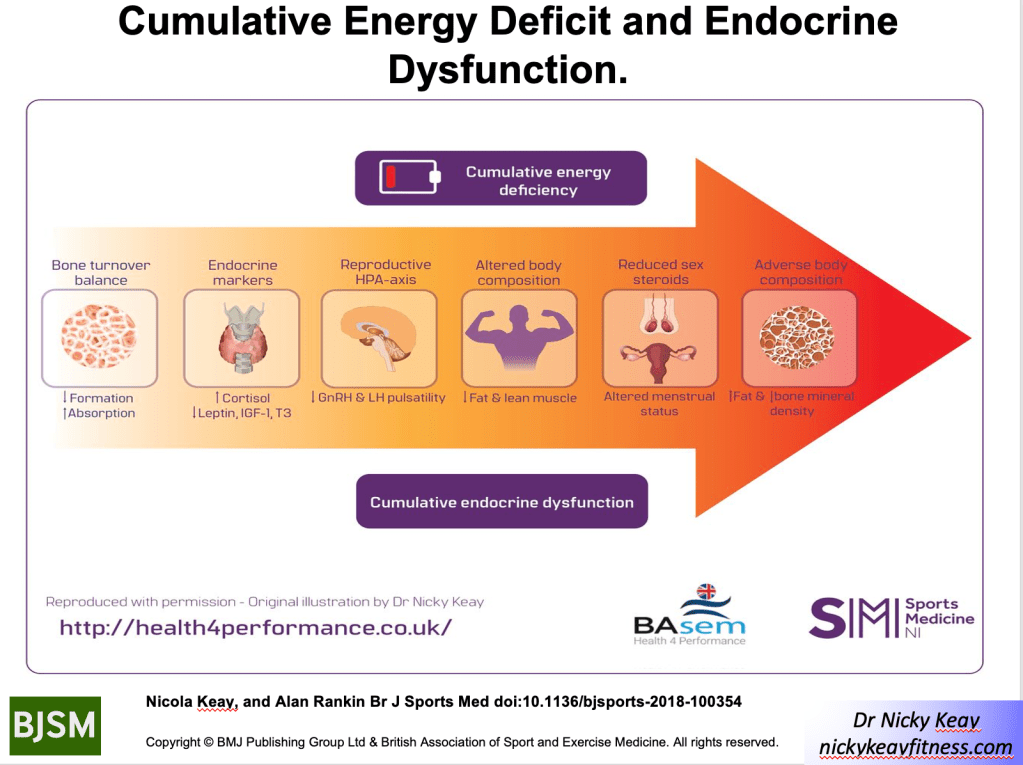
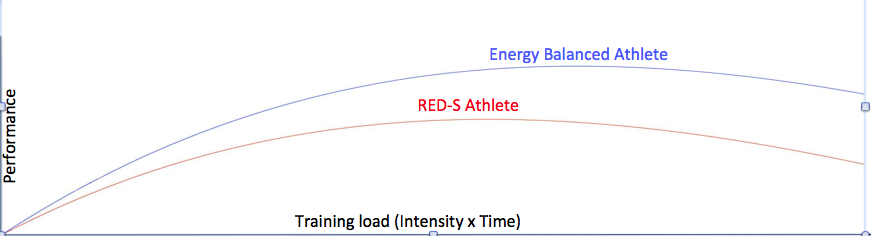
These adaptive changes across many body systems have adverse outcomes on both health and performance. This is REDs. The clinical syndrome of health and performance consequences of long-term low energy availability. This is what happened in our study of male cyclists referenced in the BJSM publication. We quantified the negative effects of low energy availability on hormone networks, bone health and performance in male cyclists[3]. Those cyclists in low energy availability lost bone mass commensurate with an astronaut in space for 6 months and underperformed in races[4]. This negative impact of low energy availability on performance was underlined in our other studies of male athletes, referenced in the IOC papers [5,6]. Ultimately these are particularly important findings for athletes and their coaches, where performance is the priority.
Menstrual cycles
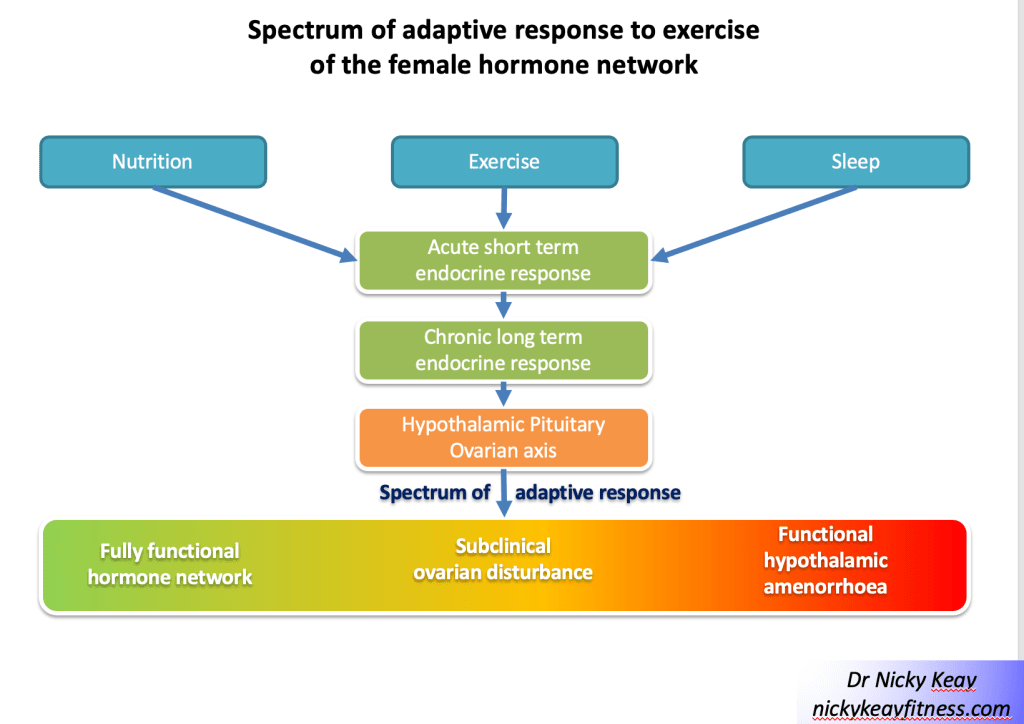
This concept of a gradated adaptive response to the combined effects of training load, nutrition and recovery can be applied when considering the spectrum of reproductive axis responses in female athletes and dancers, ranging from eumenorrhoea, subclinical ovulatory disturbances to functional hypothalamic amenorrhoea[7] shown in figure of Subclinical Ovulatory Disturbance. Functional hypothalamic amenorrhoea (FHA) is potentially just the tip of the iceberg when it comes to adaptive change to low energy availability. Report of menstruation and even signs of ovulation, may belie suboptimal production of progesterone. As progesterone increases metabolic rate, low production could be considered an early response to low energy availability. This hypothesis is currently being tested in a study of dancers, funded by the British Association of Sport and exercise Medicine.
Carbohydrate availability
Although we talk about low energy availability, the updated IOC consensus statement highlights that carbohydrate availability is the key. This is based on evidence that carbohydrate is the main substrate for exercise above a certain intensity. Furthermore, the hormones of the reproductive axis are particularly sensitive to carbohydrate availability. The IOC statement highlights studies, where despite isocaloric diets, those low in carbohydrate resulted in hormone disruption and poorer athletic performance outlined in the statement.
Health is essential for performance
Another important theme is that optimal health is a prerequisite for performance. This includes both physical and mental aspects of health. Many of the psychological characteristics of athletes and dancers can predispose individuals to developing REDs. For example, although dedication, perfectionism and motivation are laudable qualities, these can spill over into behaviours around training and nutrition. This can be associated with exercise dependence and disordered eating patterns.
If an individual is anxious about body shape, weight and food, this can have a negative health outcome. For example, in our study of dancers[8], quoted as a reference in the updated IOC statement, we found that there were significant relationships between anxiety about controlling weight and eating and missing training, and physical outcomes of low BMI and physiological health in terms of lack of regular menstrual cycles. Regular menstrual cycles in women are a barometer of internal healthy hormones. Similarly in another referenced study, we found that cognitive restraint in male athletes had an adverse effect on hormone profiles[9]. How you think impacts hormone health. This interaction is shown by the reversible arrow between psychological factors as both a driver and result of REDs shown in the updated REDs health conceptual model.
Weighty matter
Weight is a measurement of gravity, not athletic potential. Being a certain weight or body composition does not guarantee athletic success. This fact was emphasised by the lead author of the special edition on REDs on the BJSM podcast. Realistically most types of exercise will involve overcoming gravity, nevertheless, there comes a tipping point where being too light weight and/or having too low body fat means being unhealthy and compromising both physical and mental performance. Furthermore, we are all individuals so our personal optimal weight and body composition will be personal to each of us. Not the generic “lighter is faster”.
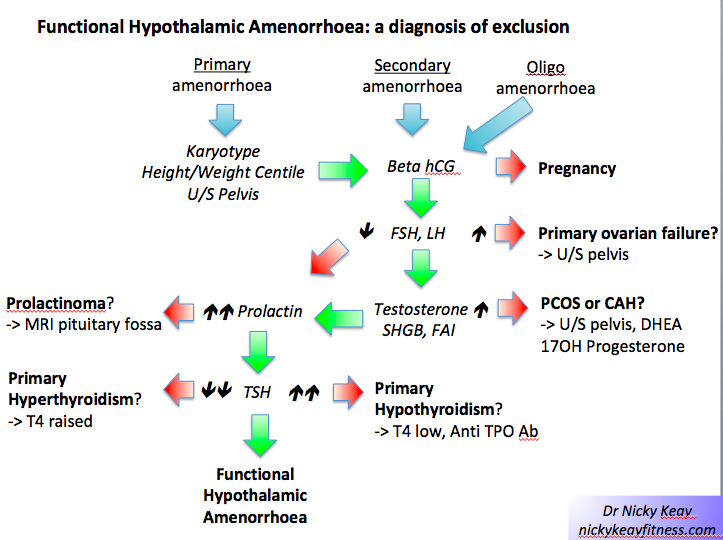
Identification
Ultimately low energy availability is a concept and not measured outside of research settings. Rather, making a diagnosis of REDs is a diagnosis of exclusion. In other words, other potential medical conditions must be excluded. This can be achieved through a process of identifying those at risk with energy availability questionnaires, followed by assessing clinical symptoms and signs: such as growth trajectories in young athletes and menstrual status in female athletes and dancers. Readily available and reliable investigations such as blood tests and DXA scans are outlined. These clinical findings have been presented as primary, severe indicators (hypothalamic reproductive disruption in men and women), primary indicators, secondary indicators and other supportive factors.
When considering hormone tests is really important to emphasise that even if a result is not out of range, where the result lies in the range is crucial. Together with considering hormones as networks providing a pattern that is informative. For example, in correctly identifying subclinical down regulation of the thyroid or reproductive axis[2].
Risk stratification
Each of indicators described in the consensus statement carries a score, so that an individual can be risk stratified. The REDsCAT2 has a finer grained zone compromising of green, yellow, orange and red, replacing the 3 zoned traffic light system.
Clinical management
Ultimately as the underlying aetiology of REDs is low energy availability, then the aim of supporting an individual experiencing REDs is to restore sufficient energy availability through a combination of nutrition and possibility reducing demand from intense training. As this will involve behaviour change, this can be challenging and a multidisciplinary team approach is advised. Highlighted for female athletes experiencing functional hypothalamic amenorrhoea (FHA) and associated poor bone health, that the combined oral contraceptive pill is not advised. Rather for bone protection in the short-term HRT (transdermal oestradiol and cyclic micronised progesterone) is recommended in line with updated NICE guidelines in UK[10].
The risk of low energy availability and REDs in dancers will be dicsuused at the forthcoming British Association of Sports and Exercise Medicine annual conference 6/10/23. https://health4performance.basem.co.uk/
References
1 An update on REDs IOC consensus statement 2023 British Journal of Sports Medicine September 2023 https://bjsm.bmj.com/content/57/17?current-issue=y
2 Keay N. Hormones, Health and Human Potential Sequoia books 2023
3 Keay N, Francis G, Hind K Low energy availability assessed by a sport-specific questionnaire and clinical interview indicative of bone health, endocrine profile and cycling performance in competitive male cyclists. BMJ Open Sport Exerc Med 2018;4:e000424. doi:10.1136/bmjsem-2018-000424
4 Keay N, Francis G, Entwistle I et al Clinical evaluation of education relating to nutrition and skeletal loading in competitive male road cyclists at risk of relative energy deficiency in sports (RED-S): 6-month randomised controlled trial BMJ Open Sport & Exercise Medicine 2019;5:e000523. doi: 10.1136/bmjsem-2019-000523
5 Jurov I, Keay N, Spudić D et al Inducing low energy availability in trained endurance male athletes results in poorer explosive power. Eur J Appl Physiol 2022;122:503–13. doi:10.1007/s00421-021-04857-4
6 Jurov I, Keay N, Rauter S Reducing energy availability in male endurance athletes: a randomized trial with a three-step energy reduction. Journal of the International Society of Sports Nutrition 2022;19:179–95. doi:10.1080/15502783.2022.2065111
7 Keay N. Interactions of the female hormone network, exercise training and nature of adaptation. ResearchGate. June 2023 DOI: 10.13140/RG.2.2.28787.71204
8 Keay N, Overseas A, Francis G Indicators and correlates of low energy availability in male and female dancers. BMJ Open Sport ExercMed 2020;6:e000906. doi:10.1136/bmjsem-2020-000906
9 Jurov I, Keay N, Hadžić V et al Relationship between energy availability, energy conservation and cognitive restraint with performance measures in male endurance athletes. J Int Soc Sports Nutr 2021;18:24. doi:10.1186/s12970-021-00419-3
10 British Association of Sports and Exercise Medicine 2023 ‘Concerning’ lack of awareness of how best to reduce risk of stress fractures in female athletes and dancers, a year after change in NICE guidelines” https://basem.co.uk/concerning-lack-of-awareness-of-how-best-to-reduce-risk-of-stress-fractures-in-female-athletes-and-dancers-a-year-after-change-in-nice-guidelines/
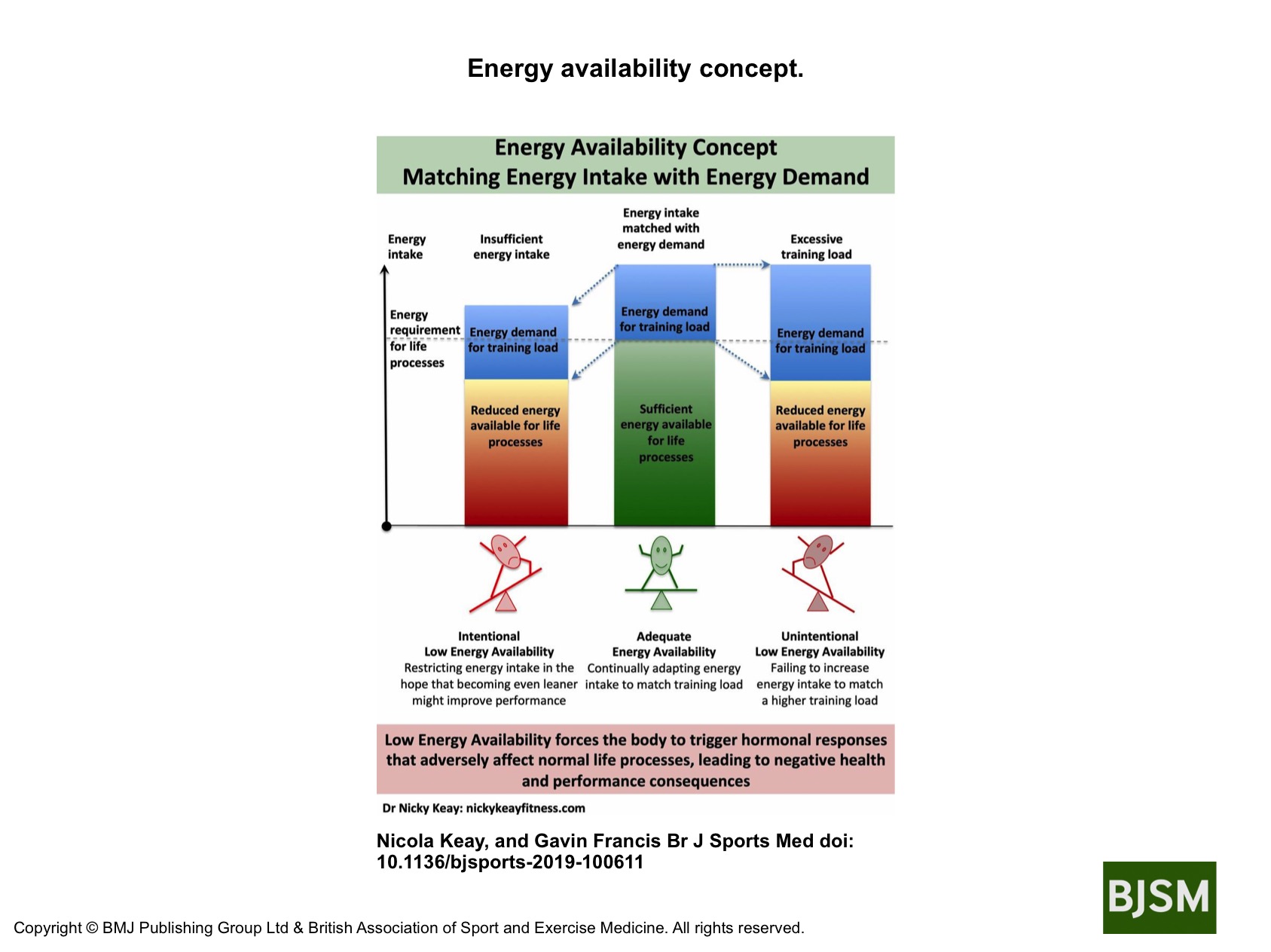



 To recap, RED-S is a situation of low energy availability (LEA), which can lead to adverse health and performance consequences[3,4]. LEA can be a result of intentional energy restriction, which covers a spectrum of issues with eating from disordered eating to full blown clinical eating disorder. Ironically the original intention of these eating issues may have been to improve athletic performance, yet
To recap, RED-S is a situation of low energy availability (LEA), which can lead to adverse health and performance consequences[3,4]. LEA can be a result of intentional energy restriction, which covers a spectrum of issues with eating from disordered eating to full blown clinical eating disorder. Ironically the original intention of these eating issues may have been to improve athletic performance, yet