Hormone Knowledge is Power
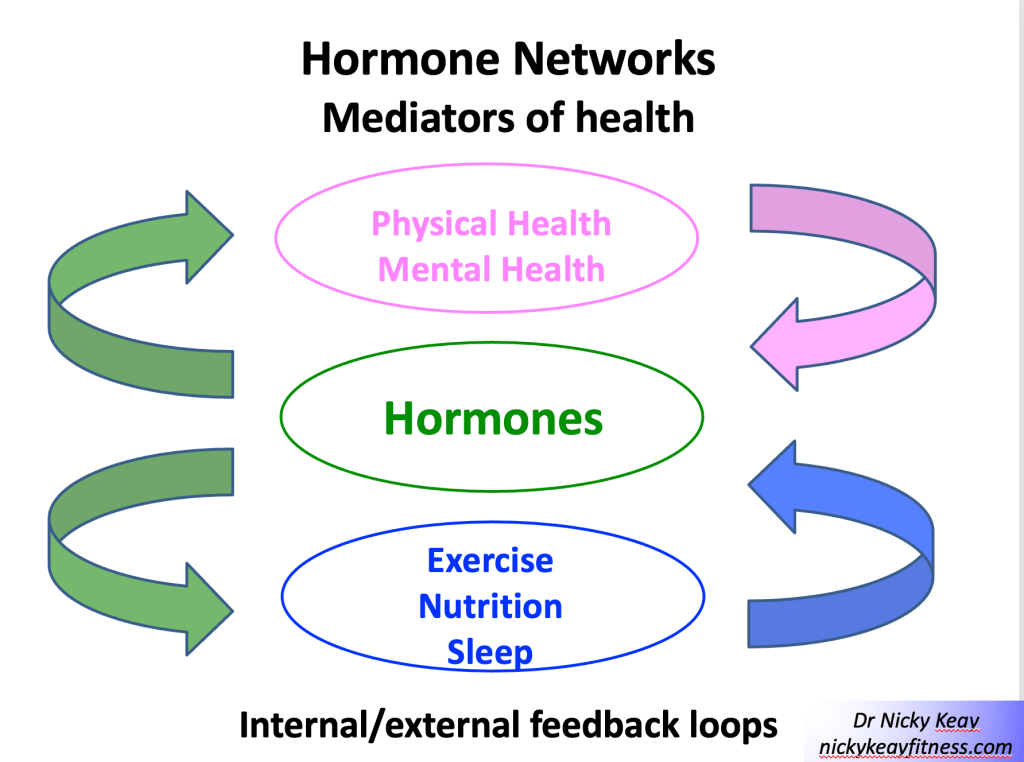
Hormones are the directors of health, enabling us to reach our personal full potential. To unlock the power of hormones and harness our hormone networks, we need to be empowered with understanding. This was the motivation for my book “Hormones, health and Human Potential: A guide to understanding your hormones to optimise your health and performance”
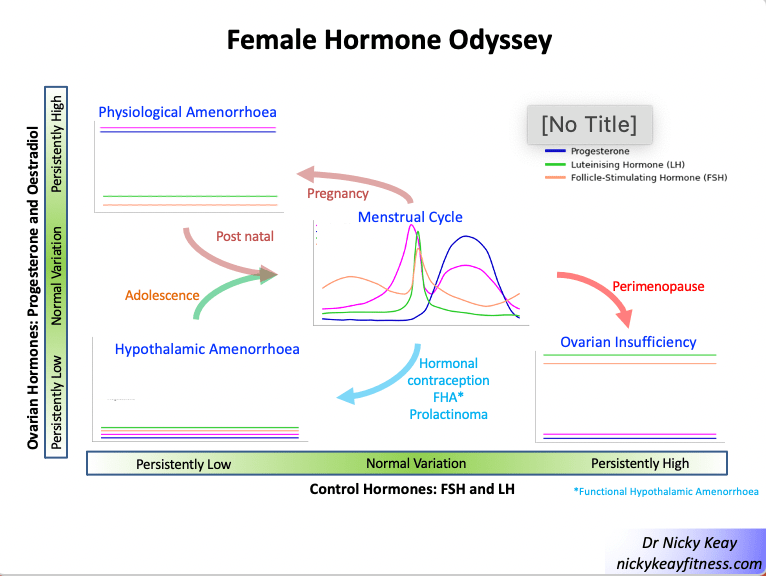
I was one of the panel discussing hormone power at Bloomfest last week. I started by suggesting that if you are ever labelled as being “hormonal”, take this as a compliment. After all, Horme is the goddess of action and energy. We discussed how to navigate the lifetime female hormone odyssey
Female Hormone Choreography
Hormone networks are complex. Out of all the networks, those of the female hormones is the most intricate. A beautiful interactive dance of hormones occurs every menstrual cycle, following characteristic choreography. However, this hormone dance will be personal to each woman, with subtleties in timing, hormone levels and crucially individual biological response. This is why knowledge is power when it comes to female hormones. Tuning into your personal variation of hormones in terms of how you feel, takes away the mystery. This empowers you to be proactive and work with your hormones, not against them. Periods are the barometer of internal hormone health and a free monthly medical check. I mentioned the potential flash points of the menstrual cycle in terms of menstruation and the luteal phase (occurring after ovulation, in the 2 weeks or so before menstruation) and practical strategies to put in place. This area is discussed in detail in Act 1, Scene 5XX “Of Mice and Men….and Women”.
Hormonal Contraception
Hormonal contraception is often an area of confusion. It is every woman’s choice regarding her personal choice of contraception. However, in order to make an informed choice about the most suitable form, it is really important to clarify the different types available. Non hormonal options, barrier methods include condoms and the copper coil. Hormonal contraception can be divided into combined (synthetic oestradiol and progesterone) and synthetic progesterone-only options. Incidentally a hormonal contraception was trialled men, but they didn’t not like the side effects. As I explain in my book, it is really important that women (and their doctors) know that combined hormonal contraception (eg combined oral contraceptive pill) and certain types of synthetic progesterone-only options, suppress the internal production of female hormones across the board. This is why these medications are very effective contraception. This suppression of internal female hormones can be very useful for women with endometriosis and polycystic ovary syndrome (PCOS) which are conditions effectively fuelled by female hormones. However, this suppression of female hormones is absolutely not suitable for women whose periods have stopped. After writing to NICE, I am pleased to report the guidelines are now updated to advise against giving hormonal contraception to women who are not experiencing periods.
Hormone Injury
Unbalanced external lifestyle choices, rather than harnessing hormones, can cause female “hormone injury”. In my book Act 1, Scene 10 “In the Red” goes into the detail of how an imbalance in behaviours around exercise and nutrition can derail female hormone choreography. I outline practical advice of how to recover from this type of “hormone injury” and what to do to restore and reboot hormone networks and return to full health.
Graduation to Menopause and beyond
Variation in female hormone choreography occurs over the longer time scale of a woman’s lifespan. Menopause is a hot topic. Although it is great to see this being discussed, I suggest we need a more positive narrative. I prefer to talk about the graduation to menopause, rather than a decline. This stage in a woman’s life is something I cover in depth in my book in Act 2 looking through the “The Seven Ages of Man and Woman”. In some cultures, being older and wiser is revered. Menopause is something that all women will experience during their life. A point in time when the ovaries retire in their production of hormones and release of eggs.
The graduation to menopause can be the most challenging. During the perimenopause the ovaries work on an unpredictable, part time basis. The female hormone choreography works smoothly in some cycles. Other cycles there will be a mistiming and confused choreography, causing some of the typical indicators of menopause. These include changes in cycle length and nature, temperature regulation issues, labile mood and brain fog being some of the most frequent. We discussed that probably the most helpful approach for women in the workplace is to facilitate discussions, sharing experiences and putting in place practical things that are helpful for the individual: for example, having a desk fan nearby, sitting near a window. From the medical support point of view, providing the facts and practical aspects of taking HRT is something that I am very pleased to be able to provide.
The quote from the Vice President of the Royal College of Obstetrics and Gynaecologists: “Treat women as individuals, not statistics” is something that resonates when it comes to discussing how to unlock and harness the power of female hormones, throughout each woman’s personal female hormone odyssey.