Hormones, Health and Human Potential
“Hormones, Health and Human Potential” explains how hormones play a crucial role in determining health. Hormone networks provide the feedback mechanism by which our lifestyle and behaviours enable us to reach our personal potential.

Introduction
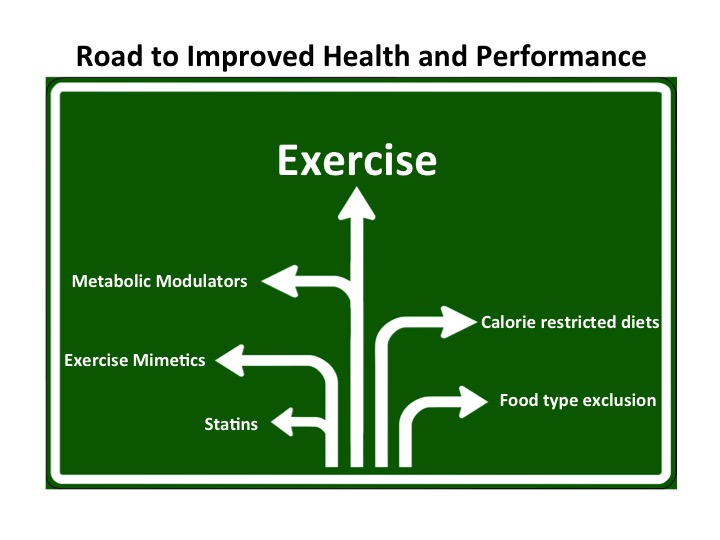
Over 2,000 years ago Hippocrates advocated that the “safest way to health” was through “the right amount of nourishment and exercise” for “every individual”. As it turns out Hippocrates was way ahead of his time in articulating the principles of personalised and preventative medicine.
Hormones as the missing link to health
Although Hippocrates understood that lifestyle and behaviours are key to health, he did not know why. We now know that hormones are the key players in this vital role. Hormones are instigators in bringing our DNA to life by determining gene expression. Hormones direct the production of proteins, in the optimal amounts and at the right time. Hormones work as networks to maintain mental and physical health.
Lifestyle factors influencing health through hormones networks
Complex internal negative feedback loops between hormones and the biological variables that they regulate, enable homeostasis for good physiological function. Challenges to homeostasis, due to our interactions with the environment are detected by the hypothalamus, which manages hormone network response. In this way there is another layer of feedback loops between lifestyle behaviours and hormones.
Well-balance lifestyle behaviours, in terms of quantity and timing, support healthy hormone network function, leading us to the “safest way to health”. Conversely, circadian misalignment, where lifestyle choices conflict between internal biochronometers, can lead to hormone dysregulation found in conditions such as metabolic syndrome.
Harnessing hormones as preventative and supportive medicine
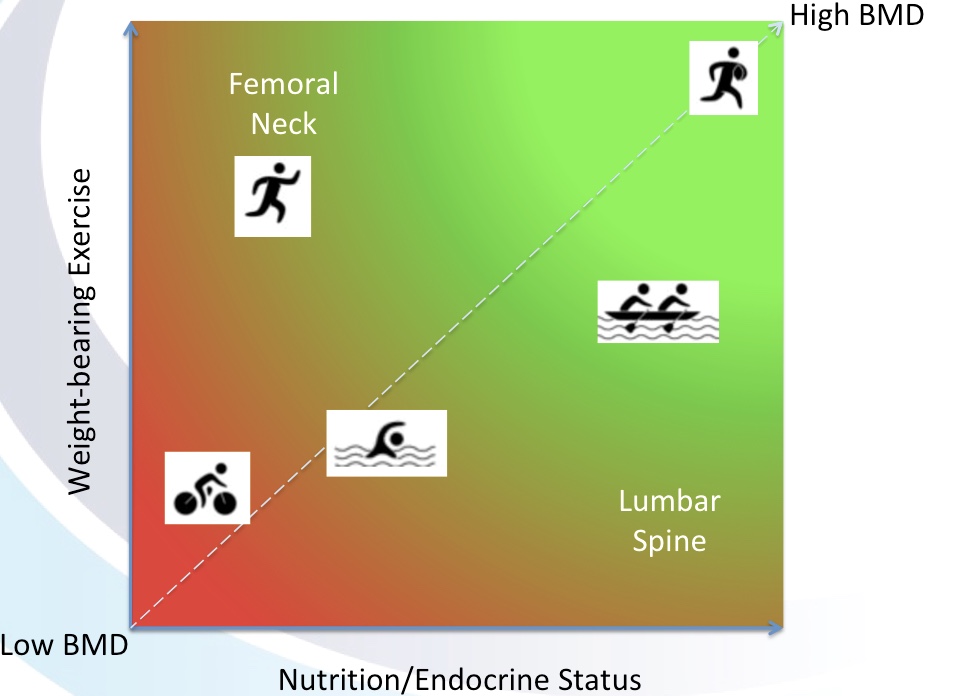
A good balance of lifestyle factors can harness hormones as a form of supportive and preventative medicine. This is particularly relevant for type 2 diabetes mellitus and metabolic syndrome. For women, where there are physiological changes in hormones, such as occurs at menopause, attendant symptoms and impacts on long term health can be mitigated by lifestyle as part of the management of menopause. For example, exercise has been shown to have a beneficial effect on temperature regulation, metabolism, body composition, bone health and reducing the risk of breast cancer.
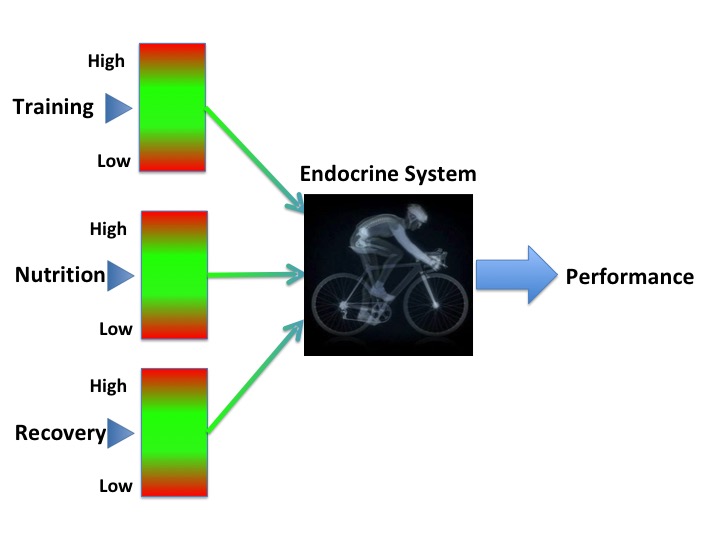
Athlete performance mediated by hormones
Hormones mediate the positive adaptive changes due to exercise training. Understanding these mechanisms can benefit both athletes and patients .
Imbalances in behaviours causing hormone dysregulation
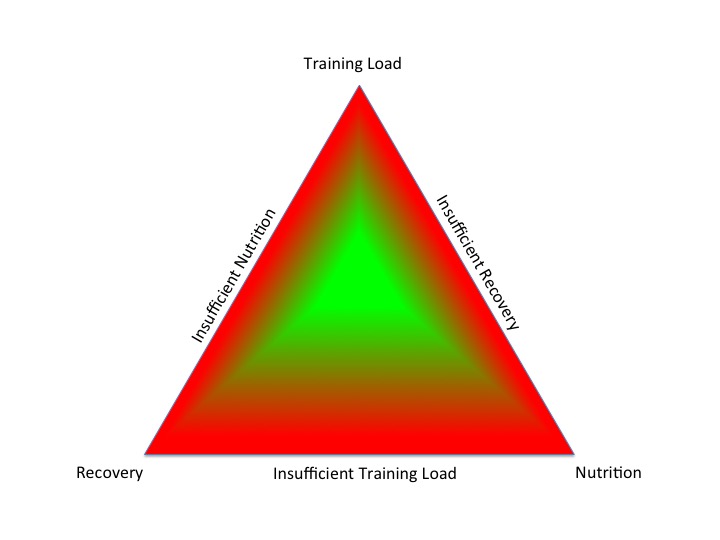
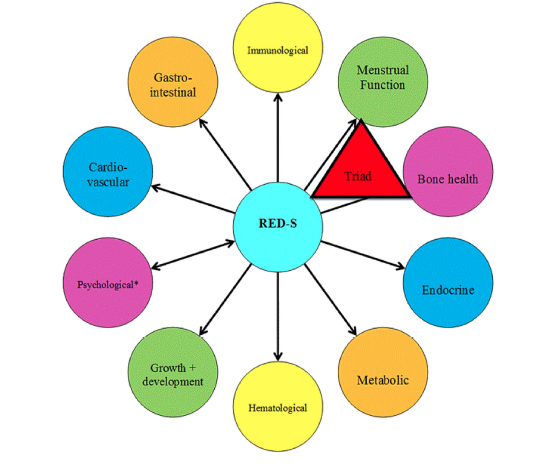
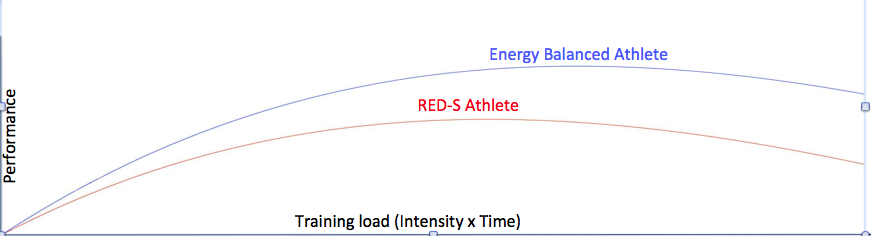
Too little exercise and excess nutrition can lead to hormone dysregulation, seen in metabolic syndrome and type 2 diabetes mellitus. On the other hand, too much of a “good thing” can also cause health and performance issues in exercisers. Relative energy deficiency in sport (RED-S) can occur in exercisers of all ages and levels, where there is either an unintentional or intentional mismatch between energy intake and energy demand. Consequent low energy availability causes hormone network disruption, which in the long-term results in adverse effects on both health and performance .
Conclusions
• Hormone network function plays an important role in mental and physical health
• Hormones are influenced by our lifestyle behaviours of exercise, nutrition and sleep
• The benefits of lifestyle behaviours are derived from the positive adaptive changes driven by hormones
• Imbalances in lifestyle behaviours can cause hormone disruption leading to adverse effects on health and exercise performance
References
Keay N. Health Hormones and Human Potential. Sequoia books. 2022
McCarthy O, Pitt J, Keay N et al Passing on the exercise baton: What can endocrine patients learn from elite athletes? Clinical Endocrinology 2022 96;(6):781-792
Keay N, Francis G Infographic. Energy availability: concept, control and consequences in relative energy deficiency in sport (RED-S) British Journal of Sports Medicine 2019;53:1310-1311.